Background: Third International Consensus Definitions for Sepsis and Septic Shock (SEP-3) defines Sepsis as life-threatening organ dysfunction due to a dysregulated host response to infection. In United States about 1.5 million Americans are diagnosed with Sepsis each year and about 250,000 of them die each year. It is also the costliest single diagnosis to treat in hospitals amounting to more than 20 billion dollars in 2013. Studies have shown that time to antibiotics more than 60 minutes after onset of severe sepsis on acute care hospital floors adversely affects patient mortality and costs of care.
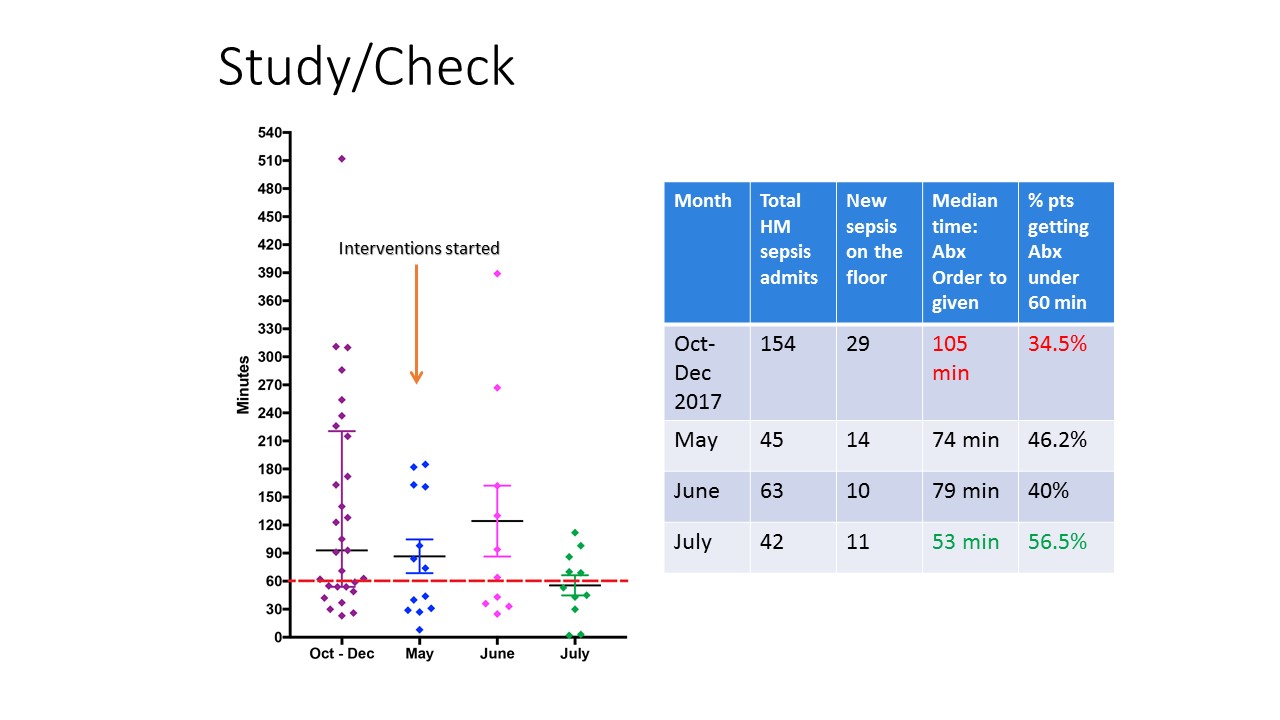
Purpose: As a part of Quality Scholars project at University of Massachusetts Medical Center, charts were reviewed of Sepsis patients admitted to the Hospital Medicine Service from October 2017 to December 2017. 19% patients (29 out of 154 patients) developed de-novo Sepsis on acute care floor when admitted for other non-sepsis related conditions. To gather baseline data, median time from order to administration of Antibiotics in Sepsis were compared between ED, ICU and floor patients. Median times were 29 minutes, 51 minutes and 105 minutes respectively. Interventions were started in May 2018 with the goal of reducing median time from Antibiotics order to administration in Sepsis patients on the floor to at least 85 minutes or less by August 2018.
Description: Currently, the provider confirms sepsis and orders antibiotic in EPIC. This starts nursing workflow and pharmacy workflow pathways simultaneously. If the antibiotic order is placed as a routine order, it can take greater than 90 minutes from order to administration. Changing this order to STAT would reduce the time significantly by providing visual cues to nursing and prioritizing the pharmacy workflow. Root Cause Analysis for delayed antibiotics showed multiple people, methods, materials and environment related issues but the significant ones addressed in this project were lack of urgency/knowledge about sepsis bundles and lack of focused sepsis order set for quick and easy use on floor patients. We used the “3 E” approach focusing on Education, building EPIC order set and Equipment (obtaining STAT IV modules/pumps). Didactic lectures were delivered to the Internal Medicine Residency, Hospitalists and Affiliate Practitioners. Educational handout and Visual Aids were posted at key locations in charting areas, Medical-Surgical floors, resident lounges and Emergency Department. A new FOCUSED SEPSIS order set was built which was presented to and approved by the hospital Sepsis Committee. The order set went live in Mid- August, so its full impact still needs to be studied. It has been well received and utilized at Health Alliance and Clinton Hospitals (part of UMass Memorial Health Care). This order set has guideline-based components of Sepsis bundles all defaulted to STAT.
Conclusions: The graphical results of median time from order to administration of antibiotics in sepsis on acute care floors during our study period of May-July 2018 is displayed in Table 1. With the above-mentioned interventions, the median time decreased from a baseline of 105 minutes (data from October to December 2017) down to 53 minutes in July 2018. Data collection from August and September was still pending at the time of completion of the Quality Scholars program. Hence, full impact of FOCUSED Sepsis order set is yet to be determined. So far, the data has looked promising and we are hopeful that with continued efforts the median time to antibiotics on floor will continue to remain under 60 minutes.