Background: Peripherally inserted central catheters (PICCs) are frequently used to deliver intravenous (IV) antibiotic therapy. Infectious disease (ID) physicians are often consulted prior to PICC placement, but whether their engagement influences PICC appropriateness and complications is not known.
Methods: Using data from the Michigan Hospital Medicine Safety Consortium on PICCs placed in hospitalized medical patients between January 1, 2015 – July 26, 2019, we examined the association between documented ID approval of PICC insertion for IV antimicrobials and device appropriateness and outcomes. Device appropriateness was defined according to the Michigan Appropriateness Guide for Intravenous Catheters (MAGIC) as a composite measure of: (a) using single-lumen instead of multi-lumen catheters; (b) avoiding PICC use ≤5 days; and (c) avoiding PICC use in patients with chronic kidney disease (defined as eGFR<45ml/min). PICC-related complications included catheter occlusion, deep vein thrombosis, and central line-associated bloodstream infection. The association of ID approval with outcomes was assessed using multivariable models adjusted for patient comorbidities and hospital-level clustering. Results are expressed as odds ratios (ORs) with corresponding 95% confidence intervals (CIs).
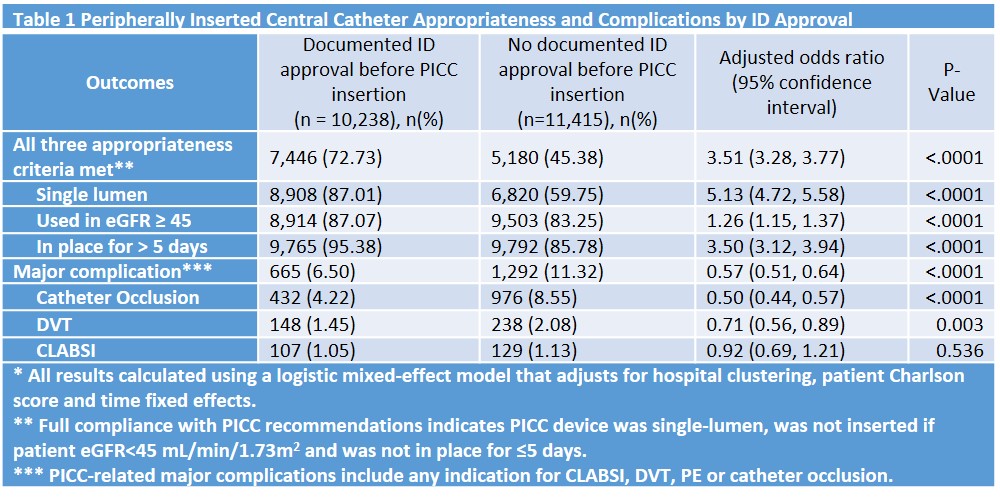
Results: Of 39,163 PICCs placed across 42 Michigan hospitals, 21,653 (55%) had an indication for IV antimicrobials and were included in this analysis. Of PICCs with an indication for IV antimicrobials, 14,935 (69%) had an ID consult prior to placement whereas 6,718 (31%) did not. Of the 14,935 PICCs with an ID consult, 10,238 (69%) had ID approval documented prior to device placement. Compared to no documented approval, PICCs approved by ID prior to insertion were more likely to be appropriate (OR=3.51, 95% CI 3.28-3.77, p<0.001). ID approval was associated with higher odds of: single lumen use (OR=5.13 [95%CI=4.72-5.58], p<0.001), dwell time >5 days (OR=3.50 [95% CI=3.12-3.94], p<0.001), placement in patients without chronic kidney disease (OR=1.26 [95% CI=1.15, 1.37], p<0.001). ID approval of PICCs prior to insertion was also associated with lower odds of PICC-related complications (OR=0.57, 95% CI=0.51, 0.64).
Conclusions: ID approval of PICC used for IV antibiotic therapy was associated with more appropriate device use and fewer complications. Policies aimed at encouraging ID assessment prior to PICC placement may help improve patient and device safety.