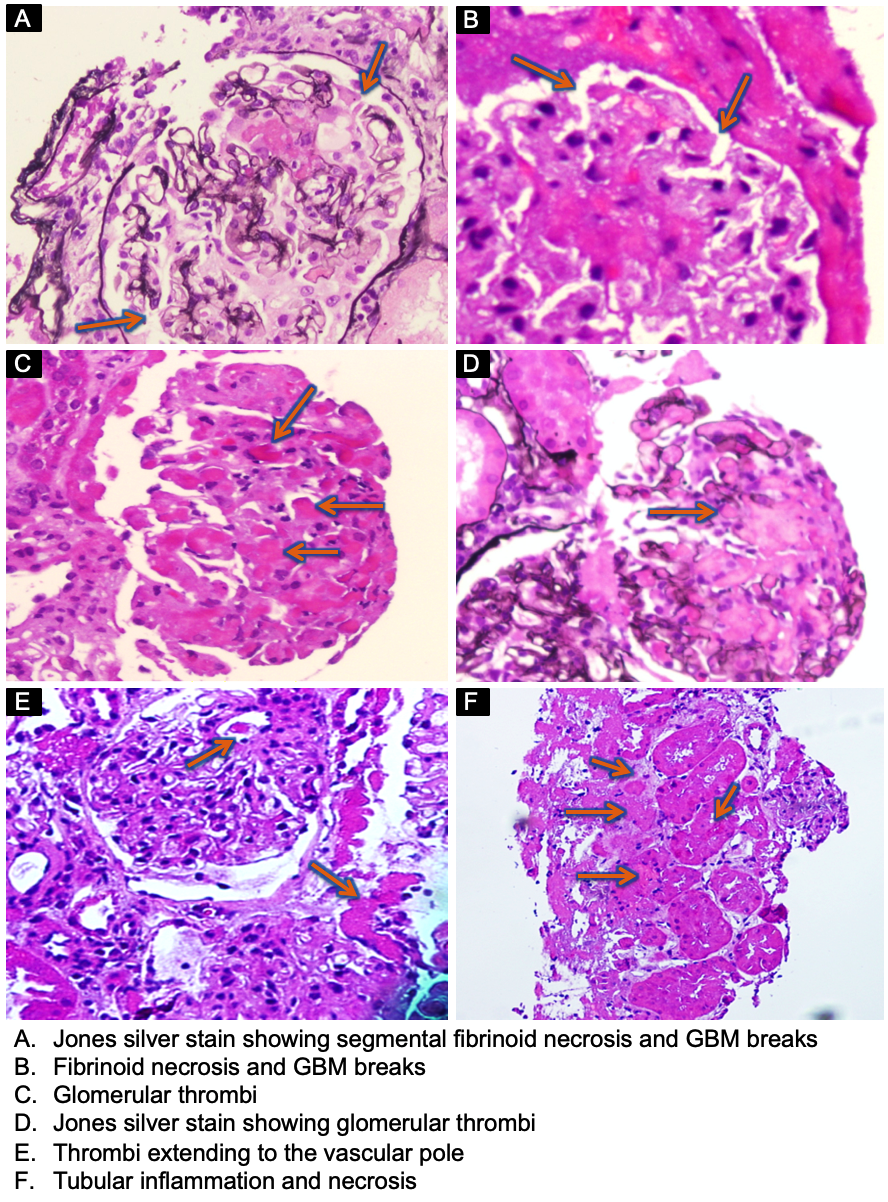
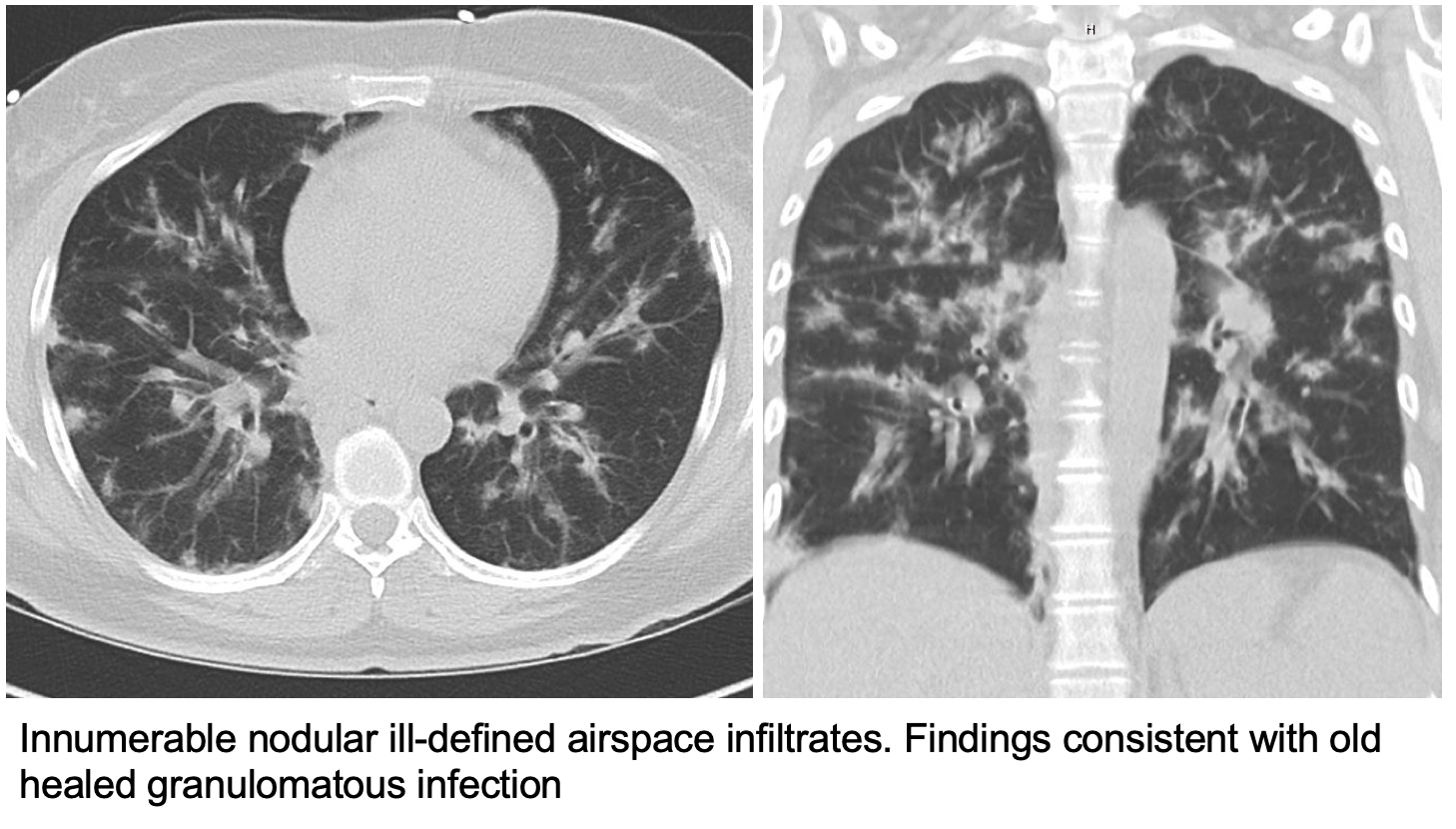
Case Presentation: A 48-year-old Columbian woman presented with 5 weeks of malaise, epistaxis, and hemoptysis. Physical exam was relevant for fever, conjunctival injection, hoarseness, coarse breath sounds, tachycardia, mononeuritis, trace lower extremity edema, and no stigmata of thrombotic microangiopathy (TMA). Labs were significant for a creatinine of 2.8, leukocytosis, thrombocytosis of 992×103, and microscopic hematuria. CT chest showed innumerable nodular airspace infiltrates and evidence of healed granulomatous infection. Renal biopsy was performed and consistent with pauci-immune necrotizing glomerulonephritis of mild chronicity, as evidenced by 10% interstitial fibrosis, crescents, and focal glomerular thrombi. PR3 was negative, and MPO antibody was positive. She was diagnosed with a MPO-ANCA positive vasculitis. Infectious workup was negative. Given the superimposed TMA, antiphospholipid syndrome was ruled out, and lupus serologies returned negative. She received pulse methylprednisolone and transitioned to prednisone and cyclophosphamide. In the outpatient setting, her shortness of breath, scleritis, hoarseness, and microscopic hematuria resolved. She is still MPO positive and steroids are being tapered.
Discussion: Renal TMA superimposed on ANCA-associated glomerulonephritis (AAGN) is a rare and unusual entity, occurring at most in 13.6% of AAGN cases. These patients present with a more aggressive renal disease. There is typically an average lag time of 9 months between diagnosis of AAGN and renal TMA, with both diseases rarely occurring simultaneously. This suggests TMA as an intermittent result of ANCA associated vasculitis flare rather than a cause of more severe glomerulonephritis. Renal TMAs are typically defined by hemolytic anemia and thrombocytopenia; however, our patient lacked these findings, suggesting the TMA existed predominantly in the renal microvasculature.Proposed mechanisms for TMA in AAGN include endothelial damage via ANCA activation of neutrophils, propagation of neutrophil extracellular traps (NETs), and alternative complement pathway activation. Due to these theorized mechanisms, plasmapheresis and eculizumab have been proposed as induction therapy for AAGN with TMA, though evidence for their use is anecdotal. Thus, high-dose induction steroids with rituximab or cyclophosphamide remains the mainstay of therapy in AAGN regardless of the presence of glomerular thrombi.
Conclusions: ANCA associated vasculitis (AAV) with renal involvement typically causes a pauci-immune glomerulonephritis due to inflammation of the small to medium sized vessels. Our patient had the hallmark features of a kidney AAV with superimposed TMA so she was aggressively treated. Due to the lack of hemolytic anemia and thrombocytopenia found on testing, we determined the TMA existed predominantly in the renal microvasculature, thus guiding the decision to proceed with traditional therapy over anticomplement drugs or plasmapheresis.