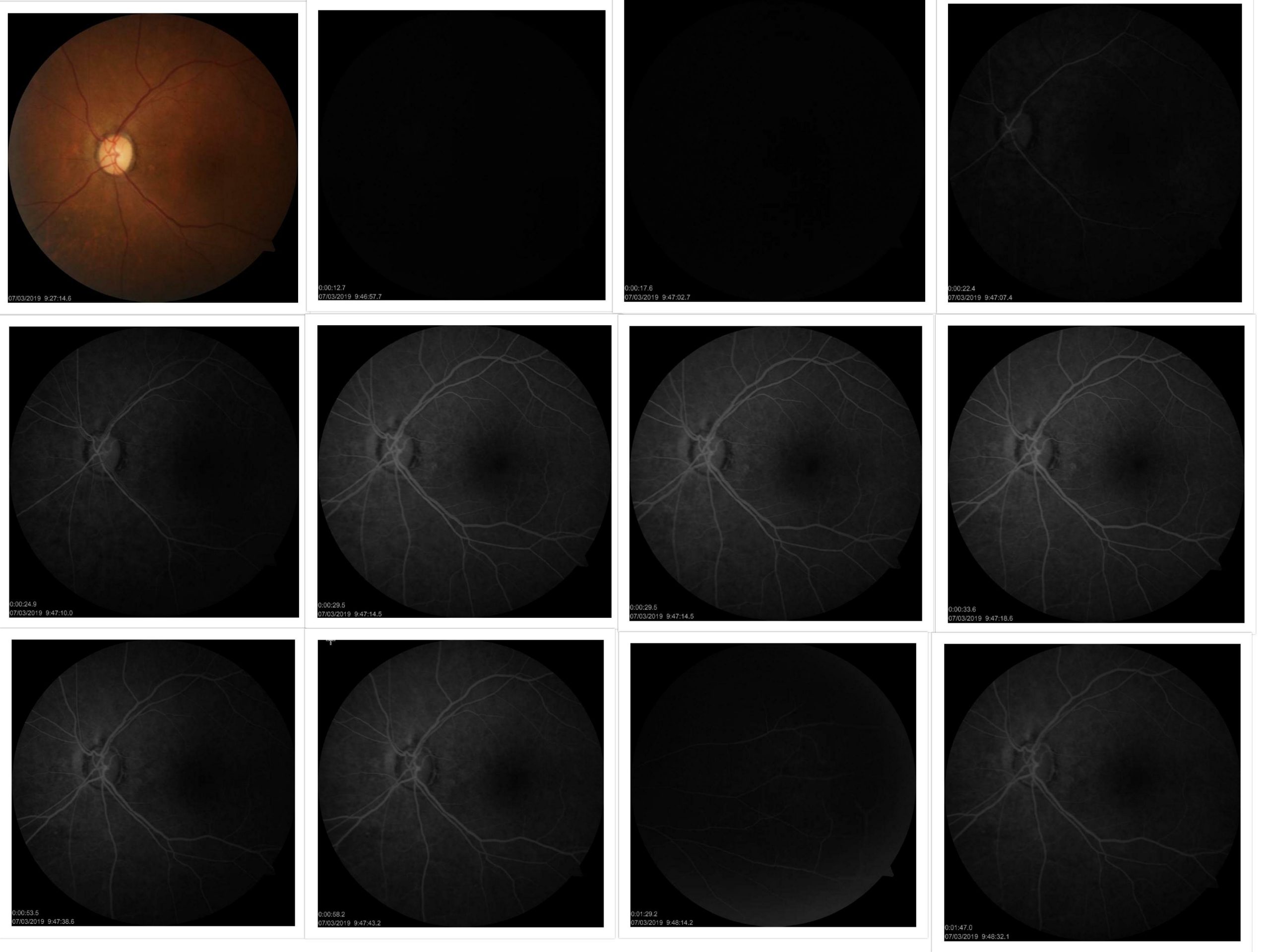
Case Presentation: A 58-year-old male presented to the emergency department with a twelve-hour history of sudden, painless and progressive left sided loss of vision following the consumption of tadalafil 20mg tablet for erectile dysfunction. He denied loss of consciousness, seizures, dizziness, headache, slurred speech, palpitations, tinnitus, urinary or stool incontinence, recent trauma, recent changes in color vision, or weakness.The past ophthalmic history is significant for two similar attacks to the affected eye following the use of sildenafil tablet one and five years ago. Initially diagnosed and treated as case of central retinal artery occlusion (CRAO). Past medical history included hypertension controlled on oral medications and erectile dysfunction. The family history was negative for both ophthalmic and systemic diseases. The physical exam showed alert and oriented male, oral temperature: 36.7 °C, RR: 17 per minute. BP: 158/84 mmHg SpO2: 99% WT: 104 kg. Ophthalmic examination revealed 6/6 vision in the right eye and close counting fingers (CCF) in the left eye. Anterior segment exam was normal in both eyes with round, reactive and regular pupils bilaterally. Fundus exam showed normal disc and macula in the right but pale disc, normal macula in the left eye. The intraocular pressure (IOP) was 12mmhg in the right and 10mmhg left eye. Investigations: The patient was admitted for workup. The patient’s ECG, routine blood tests and coagulation profile were all normal. CT head and CT angiography for the head and neck showed no abnormalities. He was advised to stop tadalafil and started on clopidogrel 75mg tablet daily. One day after the presentation, the patient reported improvement in his left eye vision. Four days after the initial presentation, the follow up ophthalmic exam of left eye showed 1/60 vision, pallor disc, sclerosed retinal vessels, retinal pigment epithelium (RPE) changes, and thinning in the fovea in addition to the admission findings. Naranjo algorithm score was: 10.Fundus photo and fundus fluorescein angiography showed normal right eye and left eye with arm-retinal flow delay (arm-retina time was 20 seconds), diminished macular capillary perfusion, and recanalized major arteries. There were no areas of abnormal fluorescence (neither hypofluorescence or hyperfluorescence), leakage or staining. (Image 1)
Discussion: Some studies reported dilatation of retinal vessels after the administration of sildenafil in healthy individulas 4. (CRAO) is serious, acute, sudden, painless retinopathy caused by the sudden decrease in the retinal layers’ perfusion. Most patients end up with vision of counting fingers (CF) or less 5. Our patient had a final acuity of 1/60 in the affected eye. Naranjo algorithm is a method used to determine the probability of drug reaction. While score equal to or greater than 9 is definite for the drug interaction 6. Our patient had his calculated Naranjo algorithm score of 10 suggesting (CRAO) as definite side effect of his (PDE5) inhibitor use. We believe that vasodilation reported in the retinal vessels after the administration of sildenafil and tadalafil causes stasis and thrombus formation which eventually leads to (CRAO). Further studies will be required to prove this association and the development (CRAO) with (PDE5) inhibitors
Conclusions: CRAO is vision threatening condition that might be associated with the use of (PDE5) inhibitors. Physicians should be aware of this serious side effect and should seek other alternativities in patients with high risk of developing (CRAO)