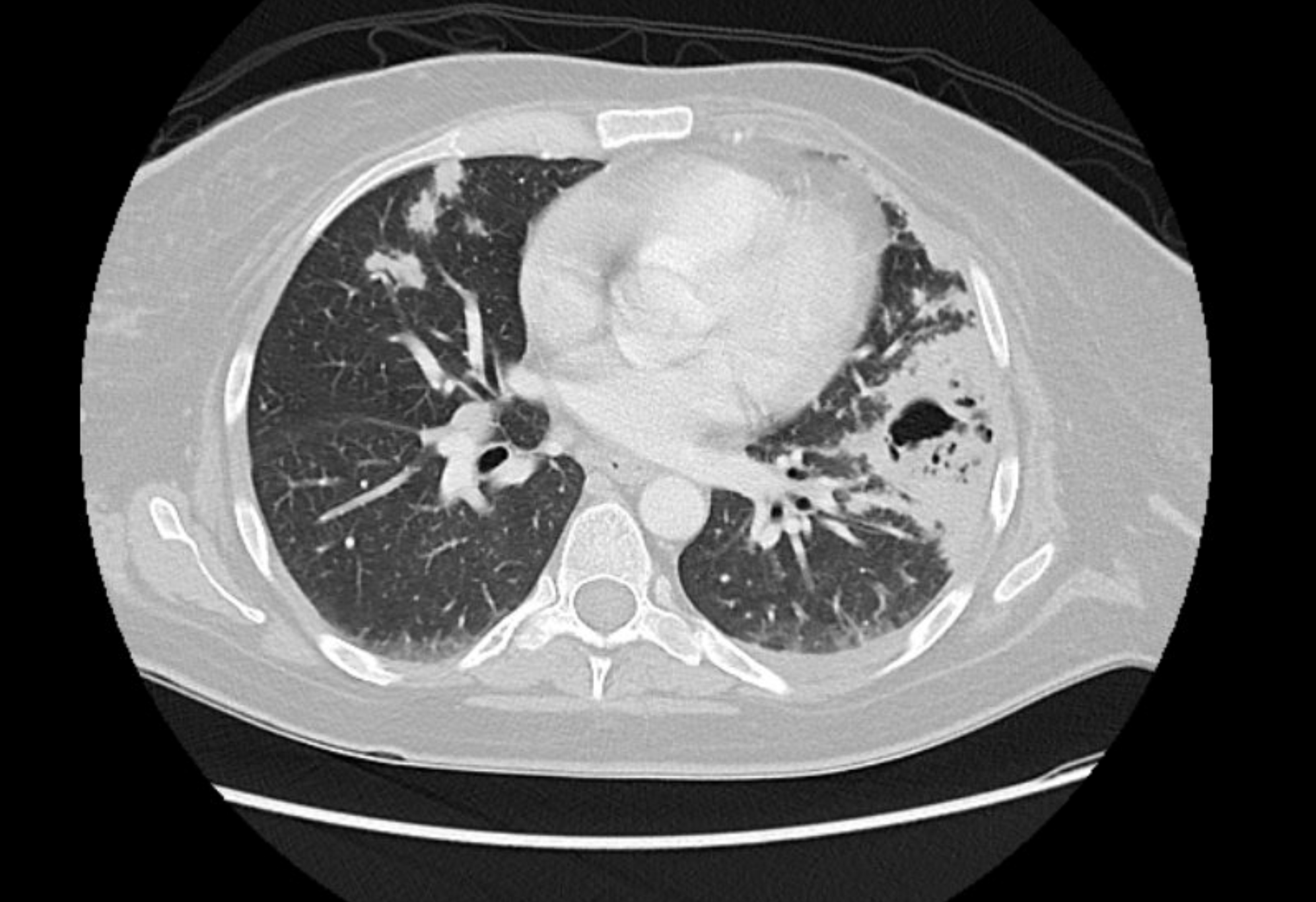
Case Presentation: A 48-year-old female with no significant past medical history was initially hospitalized for community-acquired pneumonia and subsequently developed hematemesis, melena along with fever and night sweats. Other presenting symptoms included productive cough, worsening dyspnea, and 80-pound unintentional weight loss in 3 months. She denied travel/occupation history. Further workup showed WBC 46.6×103/uL, Hemoglobin 8.3 gm/dl, and P-ANCA positive. Esophagogastroduodenoscopy showed gastritis, biopsies showed acute inflammation and ulcerations, and negative Helicobacter pylori. CT scan showed extensive bilateral pulmonary consolidation, Broncho Alveolar Lavage negative for infections, and biopsy was consistent with organizing pneumonia without vasculitis. Due to worsening lung findings and suspected vasculitis, the patient was started on prednisone 40 mg daily. The patient was transferred to a tertiary facility for a possible open lung biopsy. Repeat CT showed improvement in lung findings while on steroids. Further workup showed eosinophilia, Alkaline Phosphatase 395 IU/L, ESR 74, and CRP 4.6mg/dL, IgG at 1990 mg/dL. Colonoscopy revealed inflammation and friability in the entire colon, more prominent on the right side, perianal and rectal sparing, and no ulcers. Patient was started on infliximab due to impressive inflammatory changes in her colon. Given right-sided colon involvement and elevated Alkaline Phosphatase, Primary Sclerosing Cholangitis (PSC) was suspected. MRCP showed diffuse multifocal strictures of the intrahepatic biliary tree. Blood tests showed negative alpha fetoprotein and CA 19–9 of 76. ERCP confirmed the diagnosis of PSC with two semi-dominant strictures in the upper/lower third of the main bile duct. Biopsies of the common duct showed no dysplasia, the IgG4/IgG ratio was less than 40%. The patient was concluded to have PSC in the setting of Ulceerative Colitis (UC).
Discussion: In summary, this is a case of a patient initially believed to have vasculitis, subsequently discovered to have UC. Interstitial Lung Disease (ILD) if diagnosed, often manifests during the disease course or is attributed to medications used for UC. This case illustrates the diagnostic complexity posed due to the atypical presentation of UC reflecting an anchoring bias. Early recognition of the condition is crucial to tailor an appropriate treatment regime targeting multiple coexisting pathologies and thus preventing undue overlapping therapies with potentially severe adverse effects. It is equally important to highlight that nearly 5% of patients with UC develop PSC, which is associated with devastating complications of advanced liver fibrosis, primary hepatocellular carcinoma, and Cholangiocarcinoma. Although routine screening of PSC is not recommended, patients with UC with abnormal liver tests need immediate evaluation for PSC. This further necessitates maintaining a low threshold to obtain further diagnostic modalities, especially when the clinical picture is ambiguous, as a timely diagnosis is crucial given the high risk associated with the condition.
Conclusions: Extra gastrointestinal complications of ulcerative colitis have been well documented, although the overt parenchymal disease remains uncommon and understudied. Pulmonary findings can occur independent of UC disease activity, and thus can be the only presenting symptom of UC. This atypical presentation poses a formidable diagnostic challenge and delays appropriate and timely medical intervention.