Background: Diagnostic errors (DE) – defined as incorrect, missed, or delayed diagnoses not made within a timeframe consistent with standard clinical practice – are common and can lead to harm, especially in acute care settings. One cause of DEs is suboptimal clinical reasoning in the diagnostic process. Electronic clinical documentation has been suggested to potentially prevent DEs by facilitating the share of clinical assessments and diagnostic uncertainty between providers (1). To date, the association between the quality of documentation of clinical reasoning and the occurrence of clinically significant DE is unknown. Therefore, we conducted a retrospective cohort analysis to estimate if such an association exists. We hypothesize suboptimal documentation of clinical reasoning in admission notes of hospitalized general medicine patients may be associated with a higher frequency of DEs.
Methods: We conducted a retrospective cohort analysis of 50 patients who expired between 2016-2018 on the general medicine service at a large academic medical center (AMC) in Boston, MA. All cases underwent an institutional morbidity and mortality review process. Additionally, two clinician reviewers independently ascertained DE by conducting a structured chart review process using the SAFERDx instrument adapted for the acute setting (2). To measure quality of clinical reasoning, two different independent clinicians applied the validated CRANPL tool (3) to assess comprehensiveness of clinical reasoning documented in the assessment and plan section (A&P) of the first history and physical note (H&P) for the hospital encounter. Cases that had discordant ascertainment of DE or CRANPL scores were co-adjudicated by reviewers until consensus was reached. For cases of DE, we measured time of occurrence of the DE relative to the admission date. We used chi-squared analyses to compare whether 1) DE for the entire hospitalization and 2) DE within the first 12 hours of admission were associated with total CRANPL scores stratified by CRANPL score quartiles.
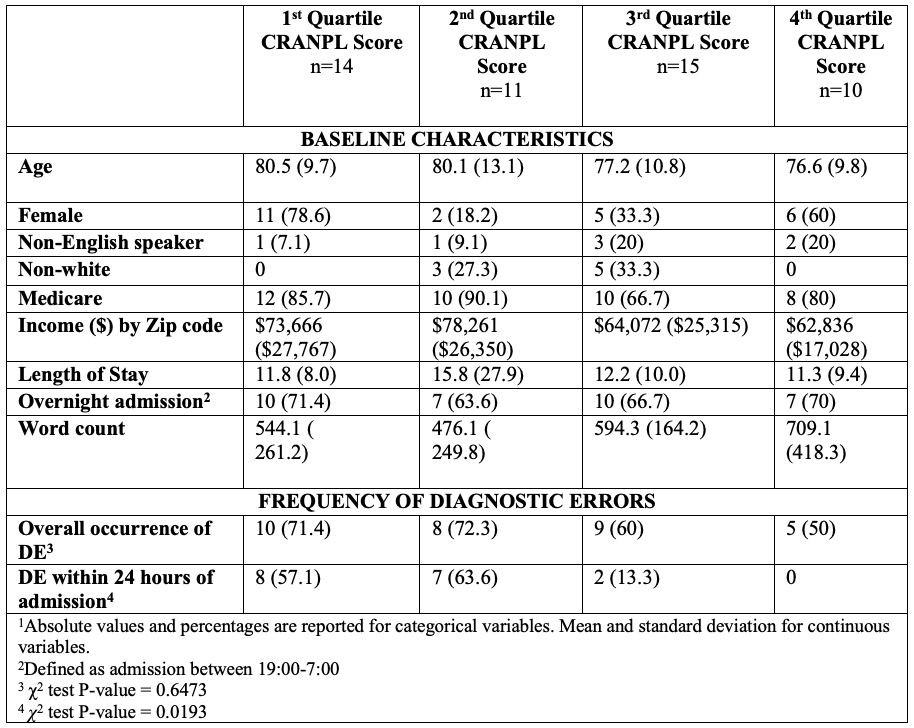
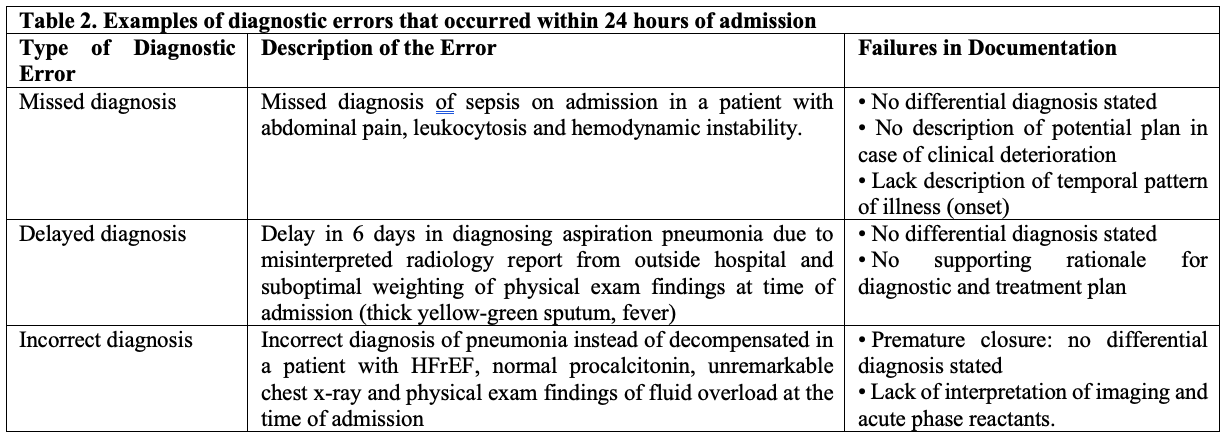
Results: Baseline characteristics are listed and stratified by CRANPL score quartiles in Table 1. CRANPL scores ranged between 5 and 14 with a median of 10.5 (IQR 8-11). Thirty-two (64%) cases were determined to have a DE by chart review; of these, DE occurred within the first 24 hours of admission in 17 cases (53%), and after the first 24 hours of admission in 15 cases (47%). There was no association between the total CRANPL scores by quartile and the frequency of DE for the entirety of the hospital encounter (p=0.68). When stratifying for DE within the first 24 hours of admission, we observed a statistically significant association between total CRANPL scores by quartile and frequency of DE (p=0.02). Table 2 shows examples of DEs that occurred within 24 hours of admission and associated failures in documentation of clinical reasoning.
Conclusions: The quality of documentation of clinical reasoning in the A&P of H&Ps may be associated with DEs during the first 24 hours following admission to the general medicine service at AMCs. Larger studies are required to confirm this finding.