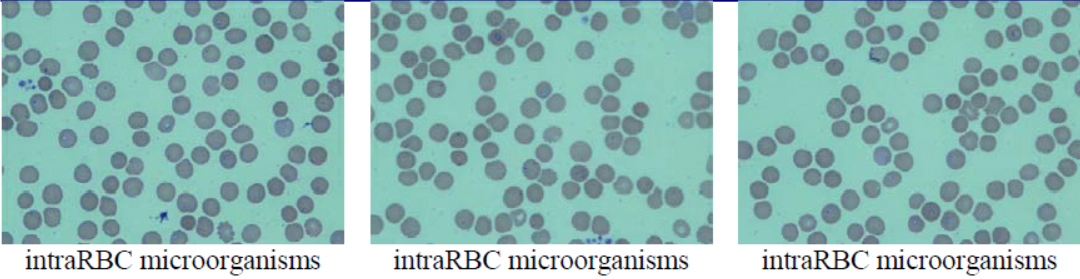
Case Presentation: A 67-year-old female presented with three days of fever, chills, and generalized weakness. She also had myalgia, epigastric pain, darker urine. She reported no recent travel but reported spending time outside gardening and walking/hiking in the woods with dogs, although she did not recallany tick bites. She had a fever of 104 °F, rigors, jaundice, and epigastric tenderness but no rash. Laboratory results significant for anemia, Hgb 9.8 g/dL, and platelet clumps, elevated creatinine 1.7 mg/dL, low sodium of 125 mmol/L, elevated AST of 73 U/L, total bilirubin of 2.4 mg/dL, lactic acid of 2.4 mmol/L, procalcitonin of 3.68 ng/mL and abnormal urinalysis (positive for large amounts of blood, bacteria, WBC, and RBC). Abdominal ultrasound and CT imaging of the abdomen/ pelvis demonstrated mild gallbladder sludge.Peripheral blood smear revealed signet ring structures in 20- 30% RBCs suggesting severe babesiosis. Further workups revealed haptoglobin <10 mg/dL, LD 1,033 U/L. Later, babesia microti DNA was detected by polymerase chain reaction (PCR), her Lyme IgG/IgM also turned positive.She was started on IV azithromycin, oral atovaquone and doxycycline. Her hemoglobin further dropped to 7.6 g/dL. She was then treated with an 8-unit exchange transfusion, and she improved with parasitemia levels decreasing (smear on the day prior to discharge showed < 0.1% parasitemia). She was discharged after seven days of hospitalization to complete 21 days of doxycycline/ atovaquone and 4 weeks of azithromycin.
Discussion: Rapid reproduction of Babesia within RBC leads to hemolysis, which can be life-threatening. Coinfections are often challenging to diagnose and lead to serious illness, causes greater disease severity and duration. Previous cross-sectional studies have suggested that coinfection is common in ticks and enzootic hosts, indicating coinfection may provide a survival advantage for both pathogens. Early clinical manifestations are non-specific and require a high index of suspicion. It is of paramount importance that clinicians should be able to recognize early signs of hemolysis and promptly exam blood smears. Along with antimicrobial therapy, the Infectious Disease Society of America recommended the use of exchange transfusion for high-grade parasitemia (≥10 percent) or in the presence of significant comorbidities to prevent further organ dysfunction and possibly death. Community education of preventive modalities, consisting of minimizing skin exposure, daily body checks, use of repellents containing DEET and protective clothing, and primary care provider awareness in endemic areas is also crucial.
Conclusions: Tick-borne diseases are endemic in the Northeastern and upper Midwest but with expanding zoogeographic location. Their presentation is non-specific and remains a diagnostic challenge, which may be a diagnostic conundrum in the current pandemic of COVID 19, which also has proteanmanifestation.