Case Presentation: A 39-year-old man presented with several days of worsening lightheadedness, fevers, and joint pains. His temperature was 99.8 Fahrenheit, pulse 122 per minute, and blood pressure 80/51 mmHg. He looked ill and uncomfortable. His palms and soles had multiple tender, purple-to-black macules and patches 3-30 mm in dimension, consistent with embolic infarcts (image 1). The left wrist and elbow were warm, swollen, and tender. No murmurs were audible. Blood cultures quickly grew methicillin-susceptible Staphylococcus aureus (MSSA). Multiple bilateral nodular densities were seen on chest X-ray, suggestive of septic pulmonary emboli. He had no other past medical history except a hospitalization after a major car accident in 2001. He did not use IV drugs.
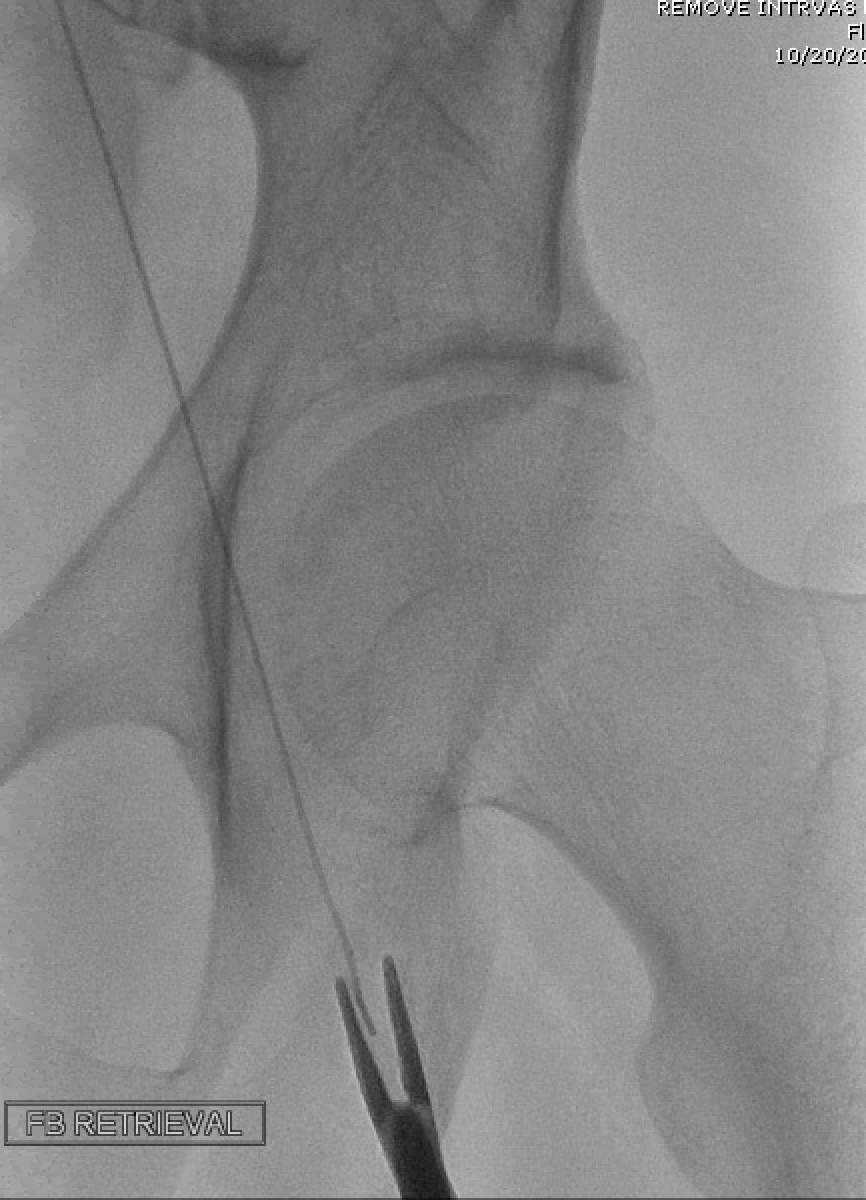
Despite appropriate antibiotics, he remained bacteremic. Suspicion for endocarditis was very high. On trans-thoracic and trans-esophageal echocardiograms (TTE and TEE, respectively), he had normal valves without vegetations, and a likely patent foramen ovale (PFO). Further imaging demonstrated a 40-cm-long metallic object running from his left femoral vein to the proximal IVC – likely a guidewire inserted and retained during treatment of his injuries in 2001. The patient underwent successful removal of the guidewire (image 2) and surgical treatment of multiple septic joints. Blood cultures subsequently cleared, and he was discharged with 6 weeks of intravenous antibiotics.
Discussion: Staphylococcal bacteremia is commonly encountered by hospitalists. Its management can involve nuanced diagnostic and therapeutic decision-making, including consideration of sources, choice and duration of antibiotics, and management of metastatic complications. This case demonstrates several of these challenges.
Trans-thoracic echocardiography is recommended in all patients with staphylococcal bacteremia to assess for endocarditis. When the pre-test probability is high, but TTE is inconclusive or negative, the more sensitive TEE must be pursued. Though there was no echocardiographic evidence of endocarditis in our patient, investigation identified an alternate narrative for his illness. The retained venous foreign body likely served as a nidus for infection and septic pulmonary emboli, while the PFO allowed for right-to-left shunting and additional systemic embolization.
Foreign bodies – most commonly central venous catheters, pacemaker wires, and prosthetic joints – can become infected in the setting of transient bacteremia. Subsequently, they can cause local complications or serve as a perpetuating source of sepsis. Successful treatment of infected foreign bodies generally requires their removal, in addition to antibiotic therapy.
Conclusions: Infective endocarditis must be ruled out in patients with staphylococcal bacteremia. When ruled out, alternate sources of persistent bacteremia and/or embolization must be established.