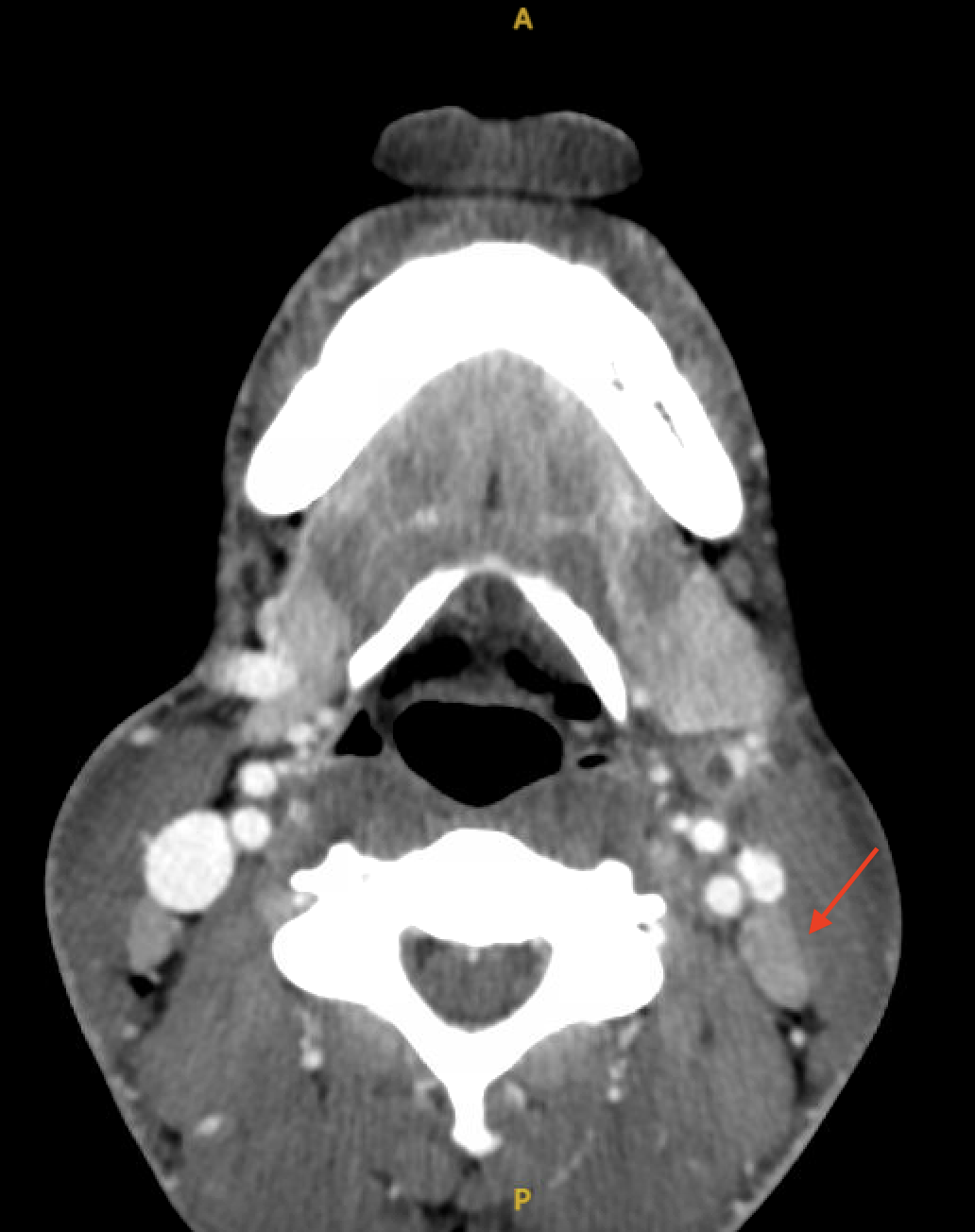
Case Presentation: A 31-year-old man presented to the ED with 2 days of fever and odynophagia, without neck pain. The physical exam was notable only for post-pharyngeal erythema without cervical lymphadenopathy. Blood cultures were drawn. The patient was discharged after reporting feeling better with a presumptive diagnosis of a viral infection. 5 days after the initial visit, he returned to the ED with the same symptoms after blood cultures revealed gram-negative anaerobic bacteremia. Upon his return, blood pressure was 84/39 mmHg, pulse rate was 57 bpm and body temperature was 36.4 °C. Uvular and tonsillar erythema, right neck fullness were noted on the physical exam. Blood tests showed a WBC count of 11.8 K/μL and a creatinine level of 2.44 mg/dL which was suggestive of acute kidney injury. The patient was admitted for management of severe sepsis with organ dysfunction. On day 1, blood cultures identified Fusobacterium species. Ceftriaxone and metronidazole were initiated. Given the presence of Fusobacterium sepsis, Lemierre’s syndrome was suspected. CT scans of the neck and chest with IV contrast revealed peritonsillar abscess, edema in the retropharyngeal and lateral neck spaces, submandibular edema, a partial filling defect in an anterior venous branch arising from the internal jugular vein, and multifocal consolidation, indicative of thrombophlebitis. The patient was transferred from floor to ICU for close monitoring of Lemierre’s syndrome with endovascular involvement. At that time, he started reporting excruciating right hip pain, rendering him unable to walk. MRI of the spine and pelvis with IV contrast showed periarticular bone marrow edema along the margins of the right sacroiliac joint, irregularity of the articular surfaces, an osseous erosion, and a right hip effusion, suggestive of septic arthritis. Arthroscopic debridement was considered. The IV antibiotics were administered for a total 2-week course. Following this, they were switched to oral amoxicillin-clavulanate for an additional 2 weeks . As the hip pain improved over the course, surgical intervention was deferred. On day 13, a repeat CT scan of the neck with IV contrast showed significant improvement in oropharyngeal, hypopharyngeal, left submandibular edema, and near-complete resolution of the left internal jugular venous thrombus. By day 14, the patient could ambulate and was subsequently discharged. A month post-discharge, his right hip pain had completely resolved.
Discussion: In this case, septic arthritis was considered a complication of Lemierre’s syndrome, due to hematogenous spread, and it responded well to prolonged antibiotic treatment. Septic arthritis is reported in about 13% – 27% of cases of Lemierre’s syndrome. The joints most often affected are the hip, knee, shoulder, sacroiliac. Many studies have suggested the early initiation of surgical management in conjunction with medical management, particularly if there are distant septic emboli or collections. For patients with Lemierre’s syndrome who experience severe joint pain, additional imaging for septic arthritis is crucial to assess possible needs of surgical intervention.
Conclusions: Due to the high rates of joint involvement in Lemierre’s syndrome, diagnostic imaging studies and empiric treatment are beneficial in patients presenting with severe joint pain. This approach is crucial for the early identification of potential septic arthritis, which significantly influences the management strategy, including the consideration of surgical interventions.