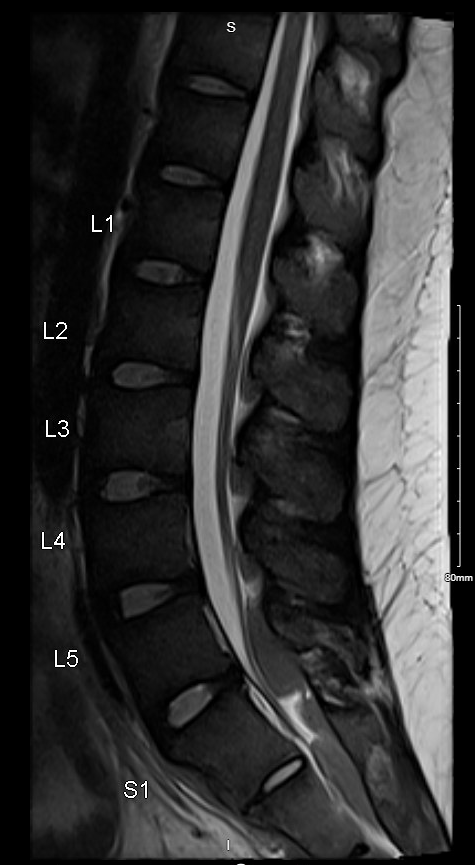
Case Presentation: 19 year old male who presented to Riverside Medical Center with acute onset, progressive bilateral lower extremity weakness and paresthesias, urinary retention and saddle anesthesia. Initial CBC significant for anemia and thrombocytopenia. Peripheral smear showed 67% circulating blasts with occasional Auer rods, which was suggestive of acute myeloid leukemia. Flow cytommetry showed expression of CD45, CD56 and aberrant expression of lymphoid antigens which may be correlated with an underlying t(8;21). MRI thoracic and lumbar spine was significant for paraspinal soft tissue masses tracking along the length of the thoracic spine, lower lumbosacral spine with extension into the bilateral neural foramina and obliteration of subarachnoid space. CT chest/abdomen/pelvis was significant for soft tissue mass in the presacral region measuring 4.8 x 3.3 cm. Patient was given methylprednisolone to temporarily relieve neurological symptoms. He was transferred to University of Chicago for further evaluation. Oncology was consulted and recommended palliative radiation initially to reverse focal neurological deficits and to minimize myelosuppression. Furthermore, he underwent induction therapy which was complicated by GI bleeding and SBO/ileus. The patient gradually improved and had a bone marrow biopsy that ultimately showed no residual AML.
Discussion: Neuroleukemiosis is the phenomenon that occurs when there is leukemic infiltration of the central or peripheral nervous system, which is a rare presentation of acute myeloid leukemia (AML). AML classically presents with symptoms related to pancytopenia (i.e., weakness, fatigue, infections, hemorrhage). This patient presented with leukemic infiltration of the thoracolumbosacral spine, causing spinal cord compression, in turn leading to bilateral lower extremity weakness, saddle anesthesia and urinary retention. A few cases of AML have been reported with this unusual clinical scenario and there are no established guidelines to diagnose or treat this presentation. Ideally, MRI imaging would be reasonable to detect any soft tissue masses that are infiltrating the spinal column, with FDG uptake on PET as well. The oncologists consulted for this case had recommended fractional radiation therapy followed by induction chemotherapy, which ultimately resolved the focal neurological deficits caused by spinal cord compression as well as the blast crisis. Finally, a biopsy is obtained to confirm the diagnosis.
Conclusions: Neuroleukemiosis is a rare manifestation of acute myeloid leukemia, which can be complicated by spinal cord compression causing neurological deficits. Although there are no established diagnostic or therapeutic guidelines, it has been shown that this presentation can be treated effectively with combination of radiation therapy with or without systemic chemotherapy.