
Background:
In our 1000‐bed tertiary medical center, codes are run by ACLS‐certified internal medicine residents who have variable clinical experience in managing a Code Blue response. Daily physician and nurse changes in the code team composition make the development of consistent skills difficult. We established a mock Code Blue program as a quality control on our emergency response procedures and to provide a forum for teaching and feedback of code team participants.
Methods:
Mock codes were designed and executed by members of our institutional critical response committee (CRC) using a programmable resuscitation mannequin. Random locations were selected throughout the hospital for the mock code and the Code Blue team was activated per usual channels. The Code Blue team was blinded to the mock code until it arrived on the scene, whereby the event was treated as an actual medical emergency. Random scenarios were programmed; thus, not all mock codes led to the same clinical result. A full debriefing of the event was conducted following the final conclusion of the code response. During the event, a group of expert observers recorded data using a standardized assessment form. Forty‐five mock codes were conducted from July 2002 to May 2007. Data were extracted from the assessment forms and tabulated as shown
Results:
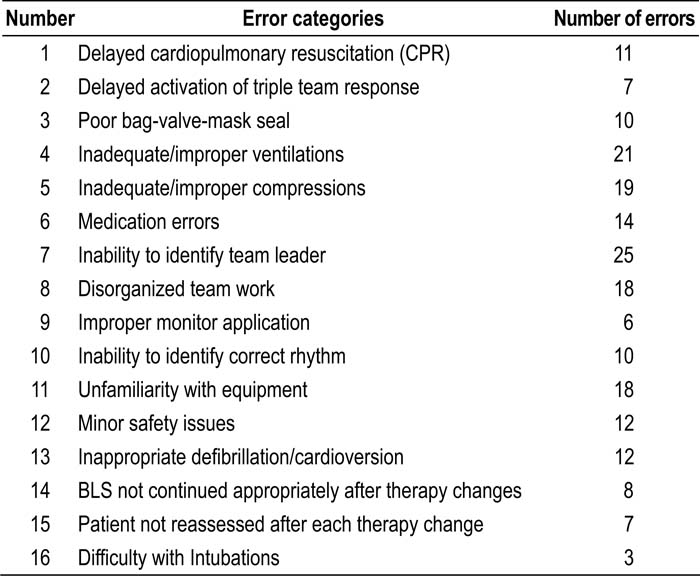
Table 1. Process Errors Identified During Mock Codes
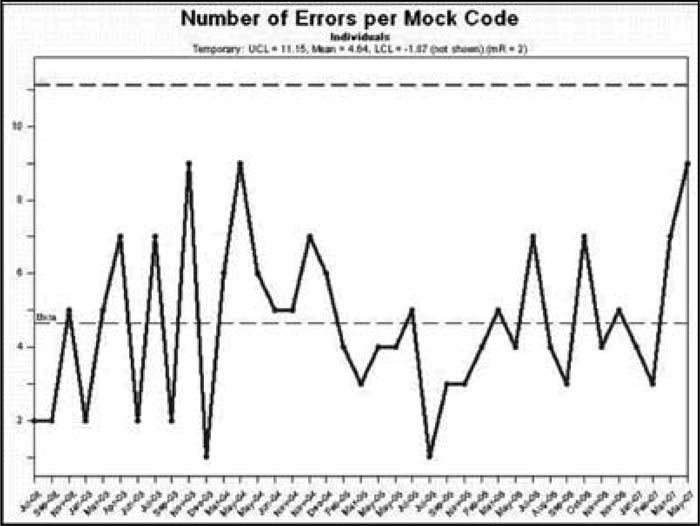
Figure 1. Mock code process errors over time.
Conclusions:
The most common theme identified in our results was the inconsistency of our Code Blue team. Most process errors did not decrease over time with our mock code program. As a quality control tool, the mock code program highlighted the impact our equipment variability had on the efficiency of our code response. This led our CRC to standardize our defibrillator equipment. Our data also reinforce the importance of a visible code team leader. As an educational intervention, all participants received feedback, and this may be expected to improve individual performance. Unfortunately, the relative importance of this education to improve outcome would be severely limited by the continuous rotation of Code Blue team members. Our mock code program suggests that a standardized Code Blue team led by staff hospitalists, not residents, may help to decrease process errors.
Author Disclosure:
A. Rajamanickam, none; D. Gugliotti, none; F. Michota, none.