Background: Discharges against medical advice (AMA) carry substantially higher risks of adverse outcomes, including a 2-fold higher 30-day readmission and 2–2.5-fold higher short-term mortality compared with planned discharges. Accurate assessment of decision-making capacity in these patients is essential, as inadequate evaluation or documentation can compromise patient safety and pose medicolegal and ethical risks. Capacity evaluations should include the four widely recognized Applebaum criteria: communicating a choice, understanding the relevant information, appreciating the medical consequences of the situation, and reasoning about treatment choices. In practice however, capacity assessment and documentation are often incomplete or inconsistent, motivating us to examine current processes at our institution. We also sought to assess clinician attitude towards capacity evaluations, perceived sufficiency of training, and interest in a standardized electronic medical record (EMR) tool to guide capacity documentation.
Methods: We retrospectively reviewed 100 randomly selected charts of patients on the general medicine service with AMA discharge orders from July 2024 through June 2025. Eight charts were excluded: four elopements, two patients who left AMA from the ED before admission, one inter-hospital transfer, and one routine discharge, leaving 92 charts for final analysis. Documentation of capacity was reviewed for the four Applebaum criteria. When the primary note was attested by an attending, their documentation was included in the review. Charts with questions or discrepancies were adjudicated by consensus among study reviewers. Additionally, internal medicine residents, advanced practice providers (APPs), and attendings were surveyed regarding their comfort with performing and documenting capacity assessments, perceived sufficiency of training, and interest in an EMR-based support tool. Responses were recorded on a 5-point Likert scale (1=low, 5=high).
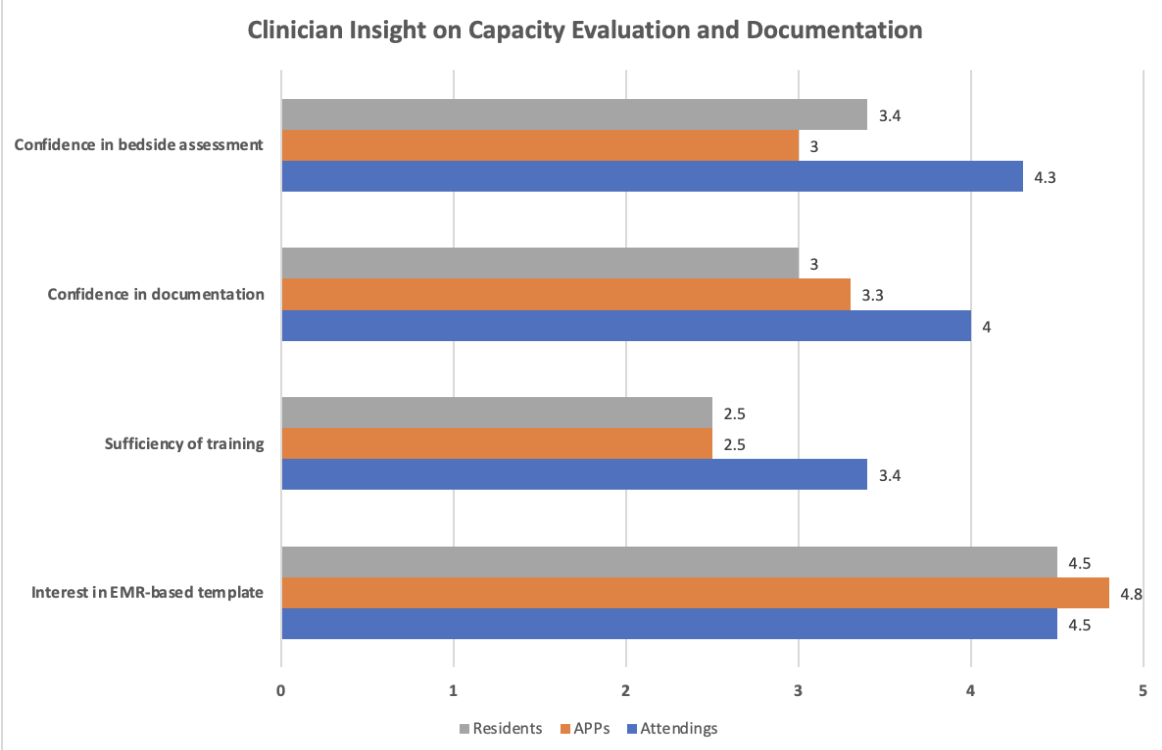
Results: Documentation of all four Applebaum criteria was complete in only 7.6% of the 92 charts reviewed; 20.7% included 3 criteria, 44.6% included 2, and 15.2% included 1. Expression of choice and appreciation of risks were most frequently documented (84.8% and 64.1%, respectively), while reasoning in support of the decision to leave AMA and understanding of the medical condition were less consistently recorded (39.1% and 12.0%, respectively). Survey responses were received from 70 of 230 residents (30%), 14 of 22 APPs (64%), and 20 of 36 attendings (56%), for a total of 104 clinicians. Residents and APPs reported moderate confidence in bedside assessments (residents 3.4, APPs 3.0) and documentation (residents 3.0, APPs 3.3), whereas attendings reported higher confidence in both (4.3 and 4.0, respectively). Perceived sufficiency of training was low among residents and APPs (2.5 each) but higher for attendings (3.4). Interest in an EMR-based template to guide capacity evaluations was high across all groups (residents 4.5, APPs 4.8, attendings 4.5).
Conclusions: Our study demonstrated that documentation of patient capacity in AMA discharge cases is properly completed in only a minority of encounters. This finding aligns with APPs’ and residents’ only moderate confidence in documenting capacity assessments and their perceived insufficient training in this area. High interest in an EMR-based support tool suggests that such a resource could be valuable in standardizing and improving documentation practices.
.png)