Background: Previous research has demonstrated missed opportunities to de-escalate from intravenous (IV) to oral (PO) antibiotics. Patients often remain on IV antibiotics longer than needed, despite known benefits of de-escalation including reduced costs and decreased risk of antibiotic resistance and catheter-associated line infections. This medical and nursing student-led quality improvement (QI) project sought to transition appropriate patients from IV to PO antibiotics through targeted provider outreach and education about an antibiotic stewardship application.
Methods: This QI initiative was conducted over five months at an urban, tertiary care hospital. Adult patients admitted to the non-teaching general medicine service who had received ≥1 IV antibiotic dose for community-acquired pneumonia or urinary tract infection with microbiologic culture and susceptibility data were eligible. Inclusion required no fever in > 24 hours and the ability to take enteral medications. Patients followed by an Infectious Diseases consultant were excluded. Student reviewers screened patients via the Electronic Medical Record (EMR) and contacted the primary attending via an EMR-based messaging platform to recommend IV to PO conversion using guidance from Firstline, an antibiotic stewardship application available to all providers. Prior to coming on service, email reminders about the initiative and Firstline were sent to attendings, and educational materials were presented during office visits and monthly faculty meetings.
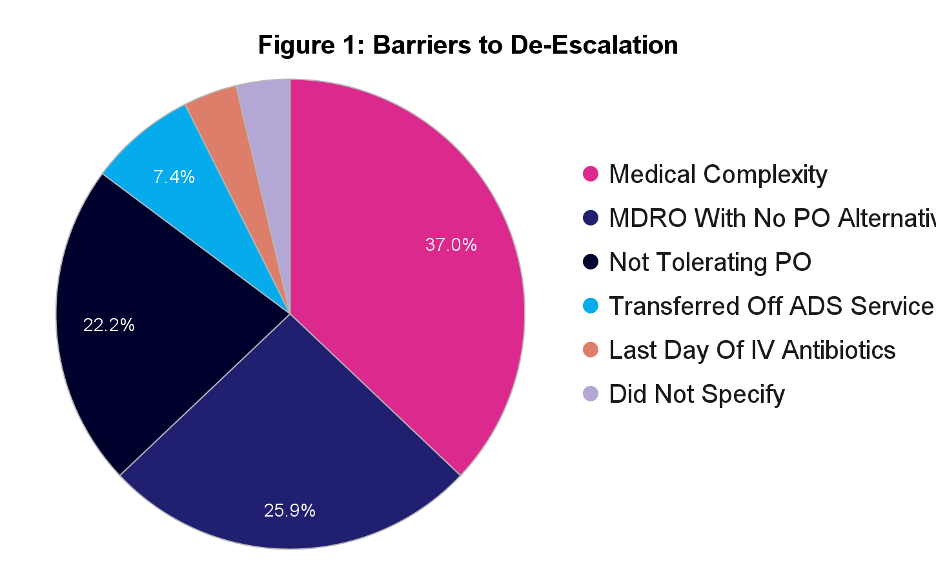
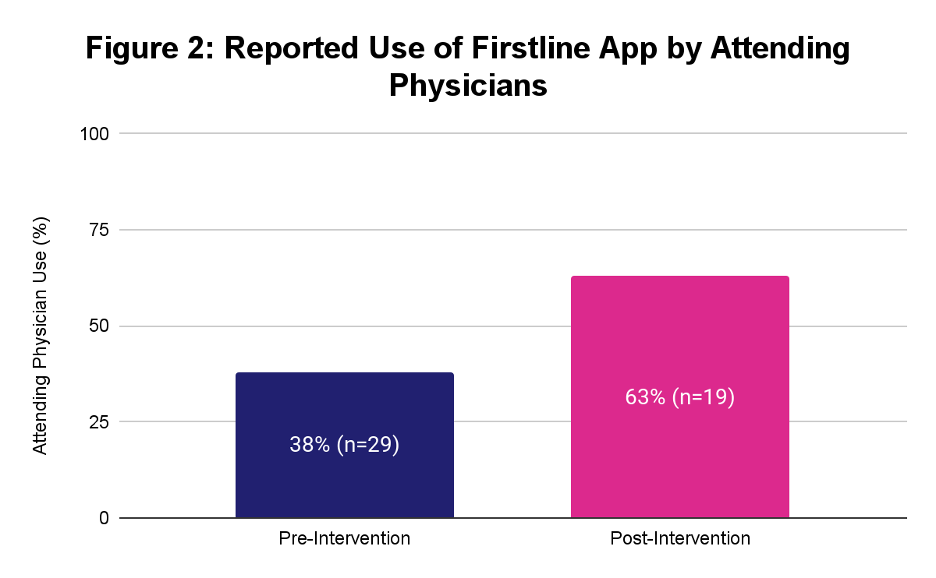
Results: Of 46 patients who met criteria, 19 (41.3%) were successfully de-escalated to PO antibiotics after provider contact by the student team. Student outreach occurred for 46 (100%) of eligible patients. 27 (58.7%) patients did not have a change in medication due to medical complexity (acuity, multiple foci of infection, lack of clinical improvement) (37.0%), multi-drug resistant organism (MDRO) with no PO alternative (25.9%), not tolerating PO (22.2%), transferred off service (7.4%), last day of IV antibiotics (3.7%), and did not specify (3.7%) (Fig. 1). Attendings were also surveyed on Firstline usage before and after the intervention. Reported usage increased from 38% (n=29) to 63% (n=19) (Fig. 2) over the course of the intervention period.
Conclusions: Targeted provider outreach and education improved IV to PO antibiotic de-escalation, with 41.3% de-escalation of included patients. Attendings reported increased use of Firstline. De-escalation was limited by patient medical complexity, MDRO with no PO alternative, and a failure to tolerate PO. These findings indicate that the complexity of patients may not be fully captured in the EMR, suggesting that relying on automation alone for de-escalation may not be a viable solution. Incorporating de-escalation into existing workflows with multidisciplinary teams (e.g. unit or team-based pharmacists) and large language models may improve the intervention’s sustainability.