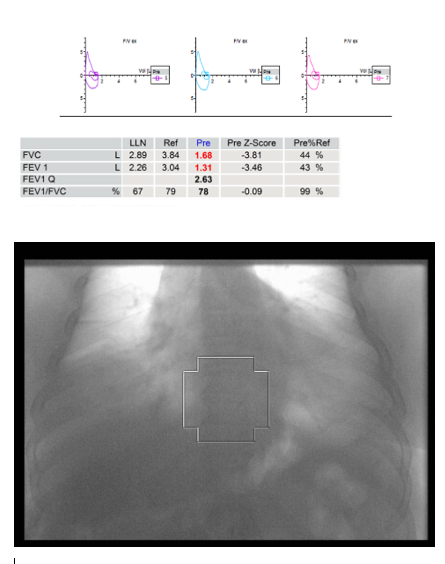
Case Presentation: A 60-year-old male with hypertension and a 30 pack-year smoking history presented with dyspnea and orthopnea. Two nights prior, he experienced profound dyspnea for 20 minutes before bedtime, worsening when supine and improving upright. The next day, he could not take a deep breath. He had mild lower extremity edema over several months. He denied fevers, weight changes, dysphagia, weakness, and vision changes. A month earlier, he could walk several miles without symptoms. On vitals he was afebrile (36.6°C), hypertensive (165/77 mmHg), normal SpO2 (96% on room air), and obese (BMI 43.6 kg/m²). Exam revealed diminished breath sounds at bases (right > left), paradoxical abdominal movement with respiration, and 3+ pitting edema around the ankles. Labs showed venous gas with a pH of 7.37 and CO2 of 54 mmHg, an elevated D-dimer (8100 mg/L) and mildly elevated CK (244 U/L). CRP, BNP, CBC, and BMP were normal. Chest X-ray demonstrated hypoinflated lungs and bibasilar opacities without effusion or pneumothorax. CT angiography excluded pulmonary embolism but upon lying flat he developed profound dyspnea and cyanosis, requiring oxygen support. Echocardiogram revealed exaggerated ventricular septal motion with normal EF and no valvular abnormalities. Bedside spirometry showed a negative inspiratory force of –40cm H2O and vital capacity of 1.2L. Bi-level positive airway support was started. Pulmonology was consulted and obtained pulmonary function tests which showed severe restriction (FVC 44% predicted, FEV1/FVC ratio of 78%). He was referred to neurology and a chest fluoroscopy revealed elevated right hemidiaphragm consistent with unilateral phrenic nerve paralysis. He improved clinically and was discharged on day 4. Ten days later, he developed ptosis, intermittent blurry vision, and fatigable chewing. Serum acetylcholine receptor (AchR) antibodies were positive (15.4 nmol/L) and he was diagnosed with myasthenia gravis with phrenic neuritis. Treatment was initiated with 60mg pyridostigmine and 4mg prednisone, later transitioned to 500mg mycophenolate due to side effects.
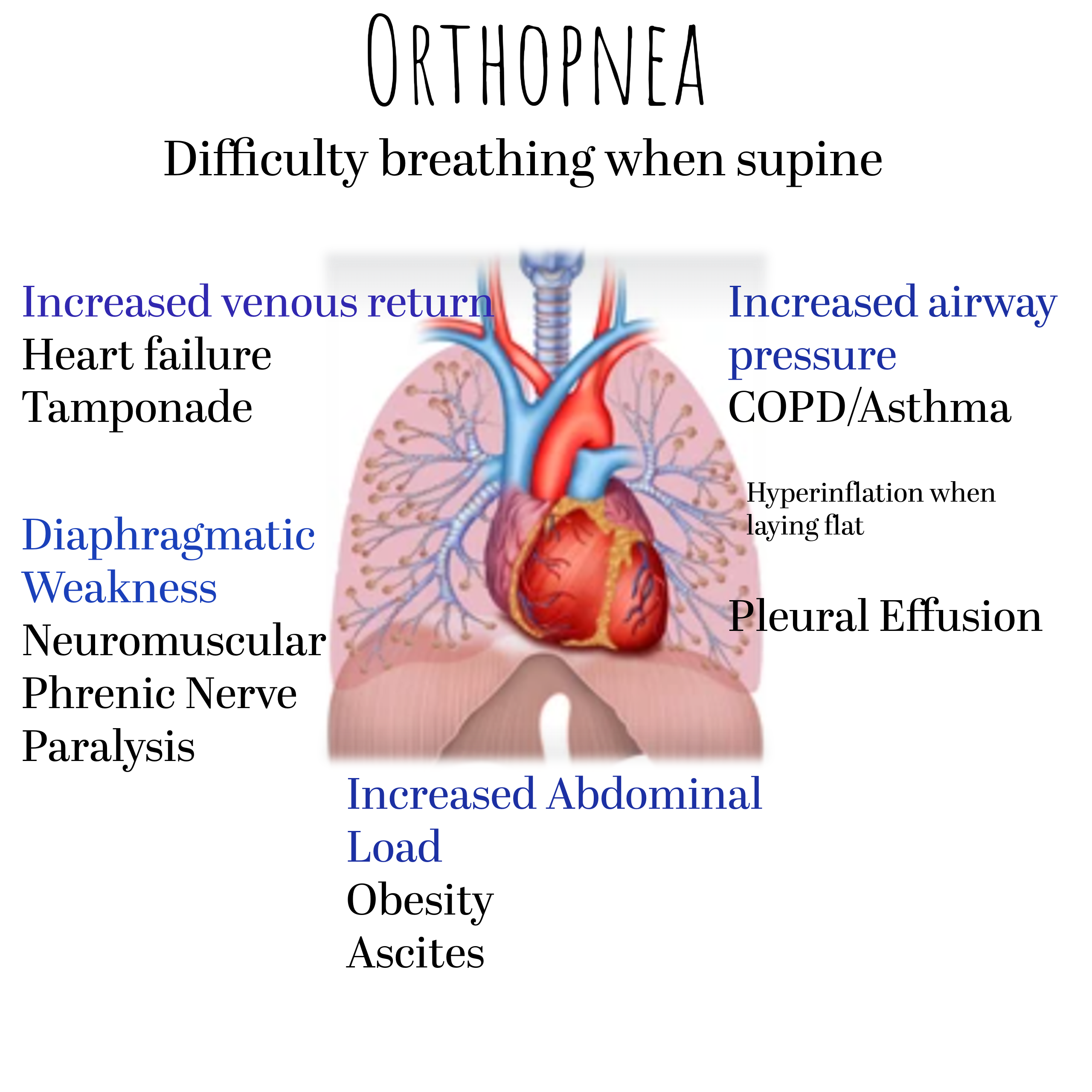
Discussion: Orthopnea is often due to heart failure, but in this case, it was a clue to neuromuscular weakness caused by phrenic nerve palsy. It is important to be aware of other causes such as increased diaphragmatic load from airway or abdominal resistance and neuromuscular weakness. Myasthenia gravis (MG) is an autoimmune disorder characterized by antibodies targeting AchR, impairing neuromuscular transmission and causing fluctuating muscle weakness1. Diaphragmatic weakness from phrenic nerve involvement is rare but can cause severe respiratory compromise, often preceding or occurring with subtle limb and ocular symptoms2,3. If persistent it may contribute to unexplained orthopnea in stable MG. Studies suggest there may be an association between MG, phrenic nerve palsy, and neuritis2,3,4. Diagnosis requires careful clinical assessment supported by imaging such as chest fluoroscopy and pulmonary function testing.
Conclusions: Phrenic neuritis causing diaphragmatic paralysis in MG is rare but potentially life-threatening. Clinicians should maintain suspicion when patients present with unexplained respiratory symptoms. In this case, not anchoring on heart failure, and evaluating for other causes of orthopnea, helped diagnose a rare condition. Timely diagnosis allows prompt immunotherapy, which may restore diaphragmatic function and improve outcomes.