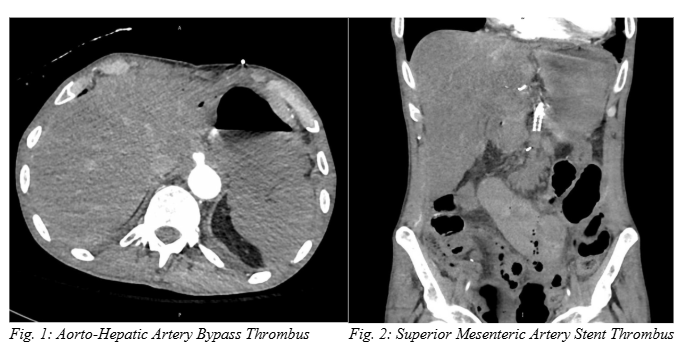
Case Presentation: A 58-year-old man with a history of chronic mesenteric ischemia status post superior mesenteric artery (SMA) stent on aspirin/ticagrelor, heterozygous factor V Leiden, and atrial fibrillation on apixaban, presented for right upper quadrant abdominal pain. One month prior, he was hospitalized for a perforated stomach ulcer, complicated by bowel ischemia status post small bowel resection. At that time, he had also undergone an aorto-hepatic/SMA bypass and SMA thrombectomy with vascular surgery. Since discharge, he continued to have persistent abdominal pain, prompting the current ED presentation. Initial MRCP showed common bile duct dilation with choledocholithiasis; ERCP was delayed for five days pending ticagrelor washout. In the interim, he was maintained on aspirin and a heparin drip, which was paused six hours prior to procedure. While he mostly only had intermittent well-controlled epigastric abdominal pain, he noted sudden epigastric pain while having a bowel movement 1-2 hours prior to his ERCP. He still underwent ERCP with successful sphincterotomy plus extraction of stones and purulence, and heparin drip was resumed six hours later. Overnight, he became hypotensive requiring vasopressors, and his abdomen was diffusely tender to palpation. His lactate was elevated to 26 mmol/L, and his CTA abdomen/pelvis revealed acute thrombosis of the aorto-hepatic artery bypass (Figure 1) and superior mesenteric artery stent (Figure 2). He underwent emergent exploratory laparotomy, however extensive bowel ischemia was found, deemed to be incompatible with life. He was transferred to the ICU where he passed away the same day after transitioning to comfort care.
Discussion: Perioperative medication management involves decisions regarding anti-platelet therapy. Guidelines for holding anti-platelets before endoscopic GI procedures vary based on bleeding risk of the procedure and underlying thrombus risk. In our patient, ERCP with sphincterotomy is high bleeding risk, while factor V Leiden is classified as moderate thrombus risk: in this case, experts recommend discontinuing thienopyridines, like ticagrelor, 5 days before procedure or switching to aspirin.1 However, our patient had also undergone prior endoscopic SMA stenting, which has high rates of re-stenosis. Studies suggest only 55-70% 1-year primary patency rate post-endovascular mesenteric artery repair2 (32% 5-year patency rate),3 with 20% of vessels having re-stenosis at median interval 0.29 years4: therefore, common vascular practice is to continue an anti-platelet agent.5 If anti-platelet agents are held in the perioperative period, recurrence of acute abdominal pain should prompt consideration of stent thrombosis with acute mesenteric ischemia, and be evaluated with CTA.6 While primarily studied in cardiac stents, intravenous cangrelor might be used to bridge while holding oral anti-platelets in high risk patients.7,8
Conclusions: We discuss a case of a 58-year-old man with recent aorto-hepatic bypass and SMA stent, and factor V Leiden, who initially presented with abdominal pain from choledocholithiasis. His abdominal pain acutely recurred due to mesenteric ischemia secondary to stent and vascular bypass thrombosis, which was likely precipitated by holding anti-platelets in the perioperative period. The risks and benefits of holding these therapies must consider procedure bleeding risk, stent/thrombus history, and other pro-thrombotic risk factors.