Background: Hospitalized cancer patients—especially those with hematologic or advanced solid malignancies—are at high risk for rapid clinical deterioration leading to unplanned ICU transfer, cardiopulmonary arrest, or in-hospital mortality. Early Warning Scores (EWS) such as MEWS, NEWS, and qSOFA are widely used on general wards, yet their performance in oncology populations is variable. Newer machine-learning (ML)–based deterioration models may offer improved accuracy, but their adoption remains limited. We conducted a systematic review to evaluate the predictive performance of EWS and ML models for detecting clinical deterioration in oncology inpatients.
Methods: We systematically reviewed published studies evaluating EWS or ML-based deterioration prediction tools among adult oncology inpatients (medical, surgical, or mixed wards). Outcomes of interest included unplanned ICU transfer, in-hospital cardiac arrest, rapid response activation, and mortality. We extracted study characteristics, model type, input features, validation approach, and AUROC values. Due to heterogeneity in outcomes, thresholds, and modeling approaches, meta-analysis was not performed.
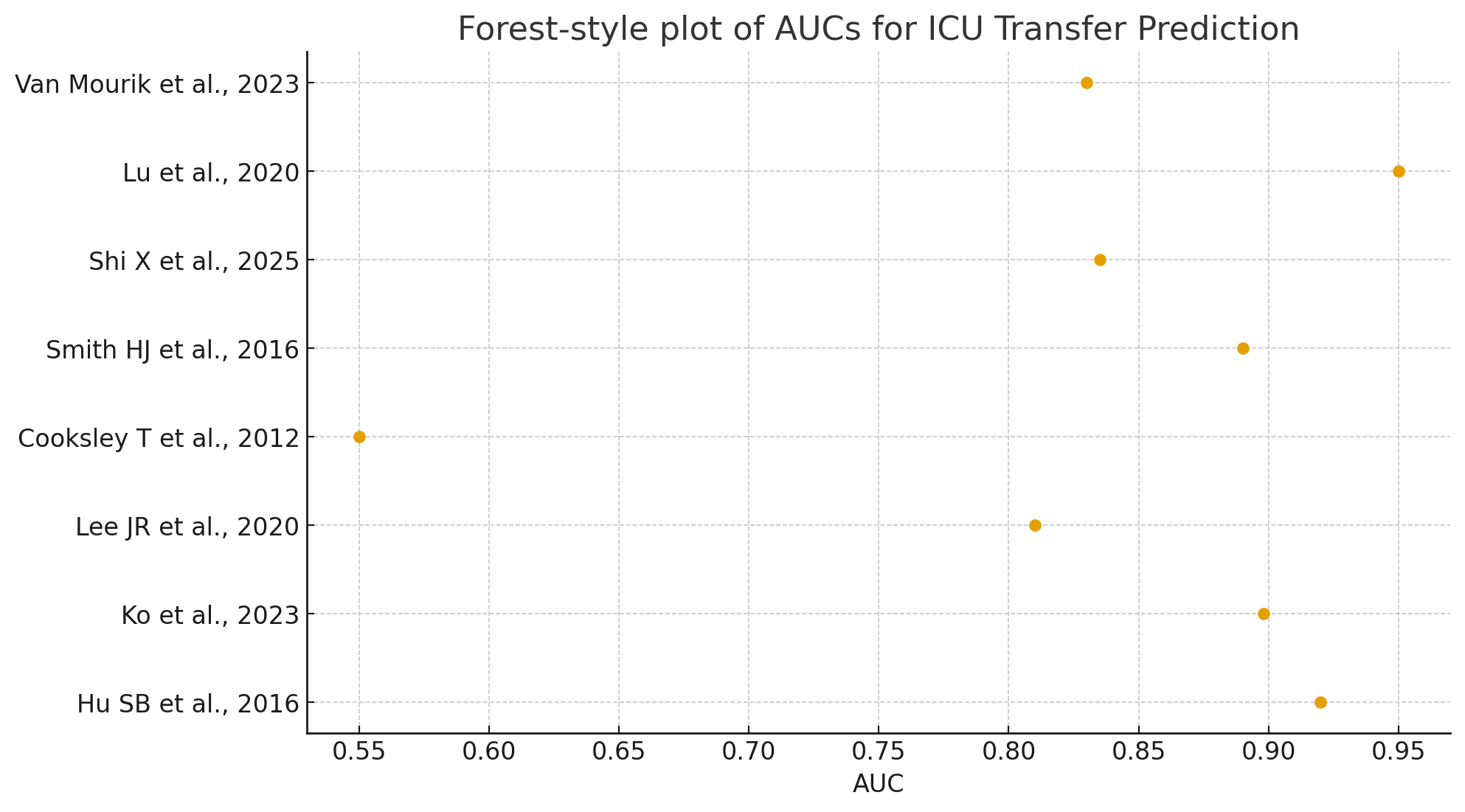
Results: Nine studies met inclusion criteria (2012–2025). Five studies evaluated traditional EWS (MEWS, NEWS, SEWS, MEWS-SF), and four studies evaluated ML models (neural networks, gradient boosting, deep-learning EWS).Traditional EWS: AUROCs ranged from 0.55 to 0.83 for predicting ICU transfer, with performance consistently lower in hematologic malignancy populations. MEWS ≥6 improved specificity but remained limited in identifying early deterioration.Enhanced EWS variants: Adding supplemental variables (SpO₂/FiO₂ ratio, lactate) improved performance (AUROC ~0.87), particularly in hematology wards.Machine Learning models: ML tools outperformed EWS across all comparative studies, with AUROCs 0.89–0.95 for predicting ICU transfer or mortality. ML models incorporated vital signs, laboratory data, medications, comorbidities, and temporal trend features.Clinical settings: Two studies focused on postoperative GI or gynecologic oncology populations; seven involved hematology or mixed oncology ward patients.Validation: Most studies used internal validation; only two used external cohorts.
Conclusions: Traditional Early Warning Scores show modest accuracy in oncology inpatients, particularly those with hematologic malignancies, where deterioration may occur rapidly and without classic vital-sign changes. Enhanced EWS incorporating respiratory indices or lactate offer improved performance, but ML-based models demonstrate the highest predictive accuracy. However, implementation barriers including limited transparency, need for EHR integration, and lack of external validation currently restrict widespread adoption.