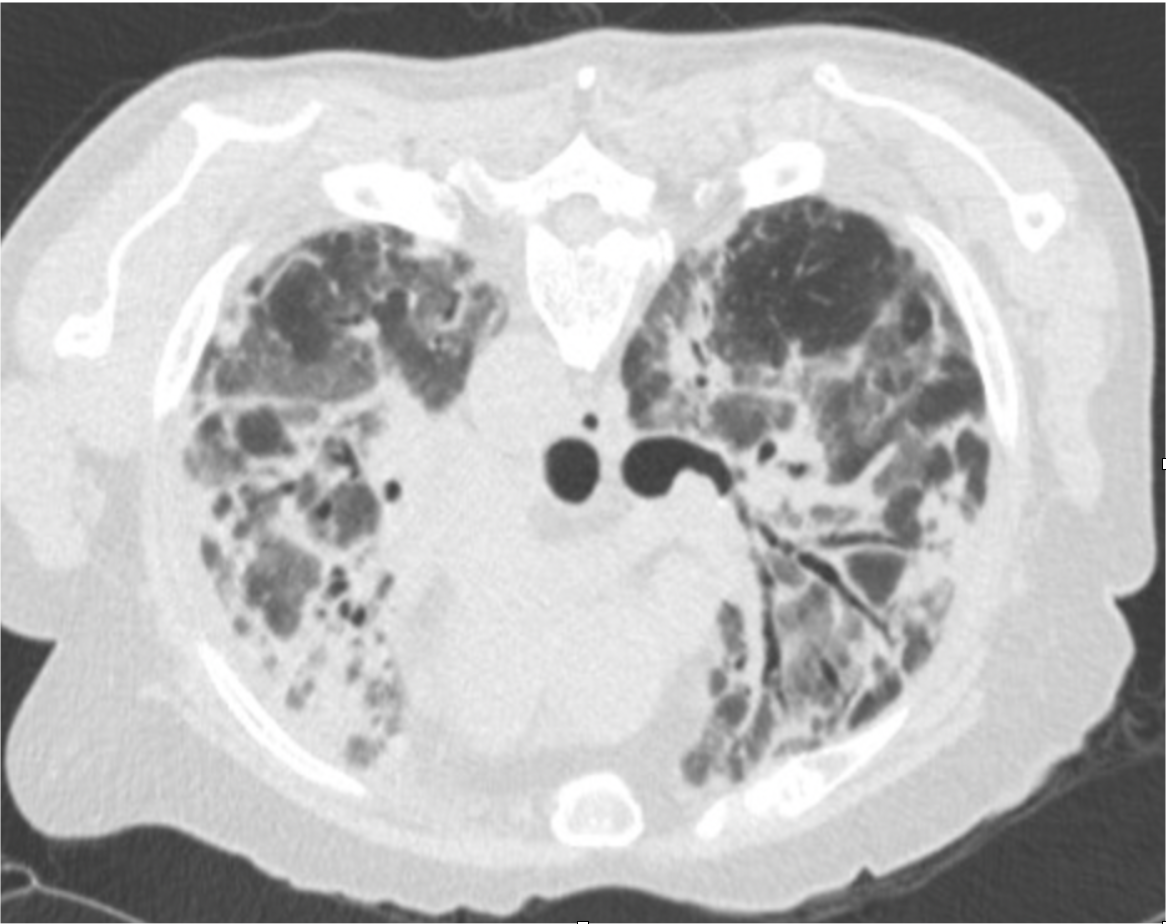
Case Presentation: A 79-year-old male with past medical history of benign prostatic hypertrophy s/p transurethral resection of the prostate (TURP) presented to the emergency department with several months of progressive dyspnea and dry cough. He was a lifelong non-smoker without chronic lung disease. Denied fevers or chest pain. On exam, he was afebrile, HR 128, RR 33 and SpO2 80% on room air. He had increased work of breathing and diffuse inspiratory crackles. Lab work was notable for WBC 13.4 x10*9/L, Hgb 13.6 g/dL and platelet count 509 x10*9/L. CMP was unremarkable and respiratory pathogen panel was negative. Elevated studies included CRP 133 mg/L and D-dimer 32,461 ng/mL. CTA of the chest showed a left lower lobe segmental occlusive pulmonary embolism and widespread fibrotic organizing pneumonia with peripheral predominance, consistent with interstitial lung disease (ILD) (Figure 1). Additional history revealed no recent or remote environmental or occupational exposures, no personal or family history of autoimmune disease, however he was started on suppressive nitrofurantoin for recurrent urinary tract infections following TURP nine months prior. The patient felt the onset of his respiratory symptoms followed the initiation of nitrofurantoin. ANA was 1:160 (speckled), but the remainder of autoimmune work up was negative. Pulmonology was consulted, and he was diagnosed with nitrofurantoin lung toxicity. Although he did have concurrent pulmonary embolism, the severe fibrotic lung injury was felt to be the primary etiology of his hypoxemic respiratory failure. Nitrofurantoin was discontinued and IV steroids were initiated. He was discharged with a 4-month steroid taper, apixiban, and home oxygen. At his 8 month follow up, symptoms were significantly improved, he no longer required supplemental oxygen, and his high-resolution chest CT showed only faint residual ground-glass opacities.
Discussion: Nitrofurantoin is a commonly prescribed antibiotic for therapeutic and suppressive treatment for urinary tract infections. Common side effects include nausea, anorexia, abdominal pain, diarrhea. Long-term complications include peripheral neuropathy, hepatocellular injury and ILD (1,2). Pulmonary complications have been well documented in the literature, however may be challenging to recognize in a hospital setting. Overall, pulmonary complications are both rare and typically mild. Nitrofurantoin related ILD severe enough to cause hospitalization has previously been observed in only 1 in 750 exposures (3). CT findings are non-specific, however a. case series of 18 patients showed bilateral ground glass attenuation with no dominant pattern of zonal distribution (4). Time course of symptom onset is variable and may be protracted: acute respiratory symptoms can develop 1-2 weeks after initiation, but chronic lung injury develops over the course of several months (5). Finally, CT findings and lab work may suggest autoimmune etiology. Literature has demonstrated, however, that a strongly positive ANA can occur in up to 60% of cases of nitrofurantoin induced ILD (2).
Conclusions: While generally well tolerated, hospitalists should be aware of potential complications of both short and long-term use of nitrofurantoin. This case highlights a rare complication of a commonly used medication and elucidates some of the pitfalls in diagnosing nitrofurantoin related ILD. Prompt discontinuation of the medication is crucial to long-term recovery of pulmonary function without recurrence of disease.