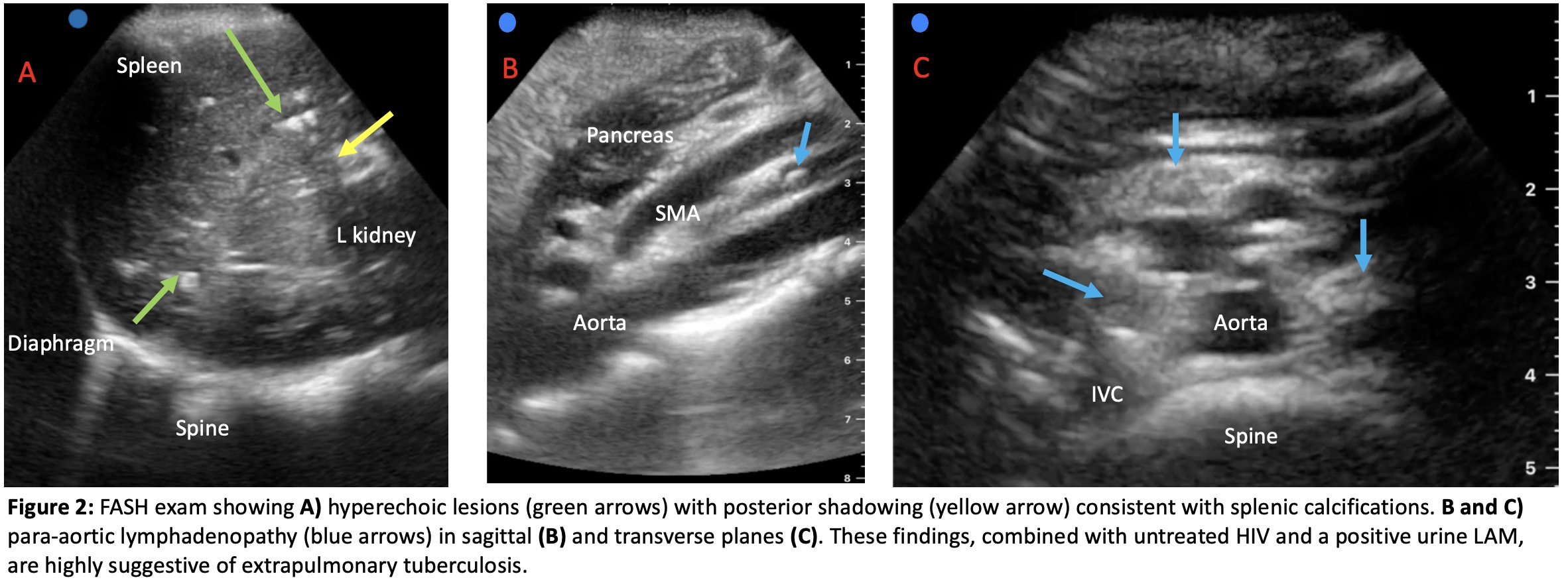
Case Presentation: A 15-year-old male with HIV and inconsistent antiretroviral therapy adherence presented to an HIV clinic in Lilongwe, Malawi with weight loss, night sweats, lower extremity rash, and diarrhea. The rash on his legs had been present for 4 months and then spread to his arms. On exam, his vital signs were unremarkable. He appeared cachectic, had no palpable lymphadenopathy, and normal abdominal and pulmonary exams. The rash consisted of hyperpigmented patches with a slightly raised and hypopigmented central aspect. Given the nonspecific physical exam, we used point-of-care ultrasound (POCUS) to perform a Focused Assessment with Sonography for HIV-associated tuberculosis (FASH) exam. This exam revealed several enlarged abdominal para-aortic lymph nodes as well as multiple hyperechoic lesions with posterior shadowing throughout the spleen suggestive of splenic calcifications. These findings, along with a positive urine Lipoarabinomannan (LAM) test and an HIV viral load of 271,000 copies/mL, were suggestive of disseminated tuberculosis (TB). The patient was started on rifampin, isoniazid, pyrazinamide, and ethambutol. He was also re-started on anti-retroviral treatment. On follow-up several months later, the patient was doing well, gaining weight, and his lower extremity rash had completely resolved with TB treatment.
Discussion: In areas with a high burden of HIV and TB coinfection, ultrasound can be very useful for the diagnosis of extra-pulmonary TB, especially in resource limited settings. The exam involves six scanning planes with the goal to identify signs concerning for extrapulmonary tuberculosis. These signs include pericardial effusions, pleural effusions, ascites, free pelvic fluid, enlarged abdominal lymph nodes, and focal liver and splenic lesions. In our patient, pertinent findings included enlarged para-aortic lymph nodes and multiple hyperechoic lesions throughout the spleen consistent with splenic calcifications. Calcified splenic granulomas are a finding that result when splenic microabscesses heal. The most common etiology of these findings in areas with high HIV prevalence are TB and histoplasmosis.Cutaneous manifestations of TB are relatively rare. Our patient’s rash appeared most consistent with tuberculids, which is a hypersensitivity reaction to mycobacterial antigens. Resolution of the rash with initiation of TB treatment further supports this diagnosis.
Conclusions: Point-of-care ultrasound can provide valuable information to the diagnostic evaluation of patients with many different pathologies. POCUS is especially useful in resource-limited settings, where other imaging modalities and diagnostic testing may be unavailable. The FASH exam describes a protocol to identify abnormal signs suggestive of extrapulmonary TB in areas where the prevalence of HIV/TB coinfection is high. Our ultrasound findings of calcified splenic granulomas and enlarged abdominal lymph nodes in a patient with HIV was highly suggestive of TB and expedited appropriate treatment.