Background: Critical illness requires initiation of several classes of medications to treat or prevent different conditions. These include nebulizers, PPIs, antipsychotics, antibiotics, steroids, anticoagulants, opioids, benzodiazepines, & several others. Continuation of these medications upon transfer from MICU to the floor is a common occurrence with downstream implications including side effects or potential harm to patients, cost, & impacts on workflow.
Purpose: The Medication Reconciliation Upon ICU Transfer (MERIT) QI initiative aims to create a formal medication reconciliation process upon transfer of patients from the MICU to the floor to improve patient handoff & ultimately de-escalate these medications.
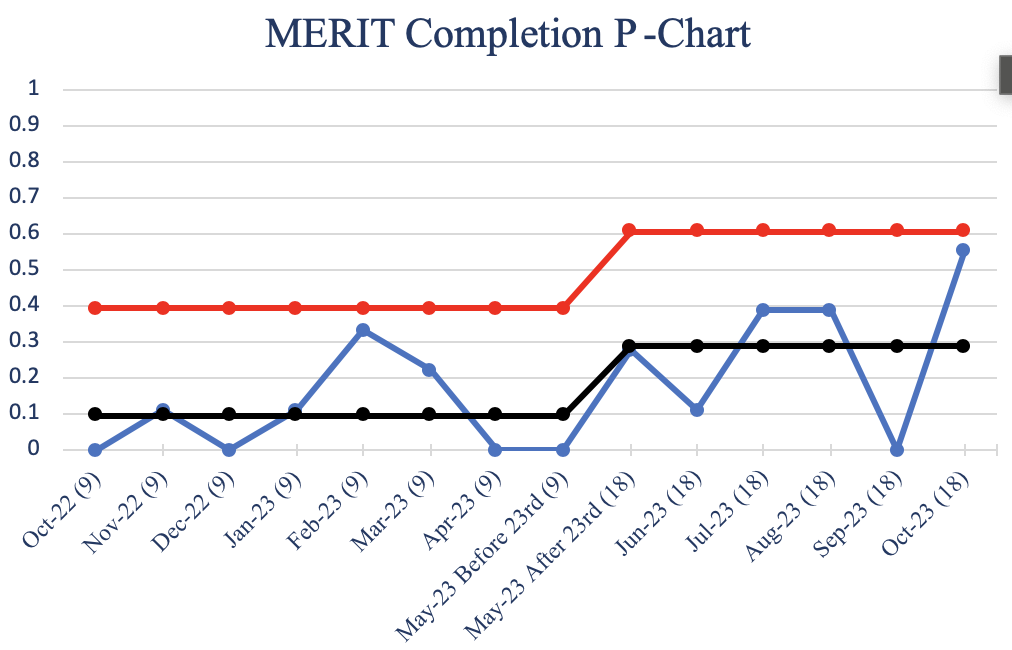
Description: Methods: PDSA cycle 1 ran from October 2022 to May 2023. After patients eligible for transfer from the MICU to the floor were identified, MERIT involves the creation of a significant event note in the Epic EMR after multidisciplinary discussion of these medications. The note is created by MICU fellows using a Smart Phrase that auto-populates these medications & highlights a plan to wean these medications on the floor as able. PDSA cycle 2 involved starting a MICU orientation for fellows & residents that mentioned MERIT to improve awareness, emphasized the process during rounds, & expanded the role of who documents the MERIT note to MICU fellows & pharmacists. PDSA cycle 2 began May 2023 & continues into the present. During each PDSA cycle, VOC, RCA, & random chart review was conducted to analyze the completion rate of the MERIT note. Stakeholders include MICU & general medicine floor attendings, fellows, residents, pharmacy, RTs, & nurses. Notable exclusions include charts of deceased patients during that admission, those admitted at the time of chart review, confidential charts, & those discharged directly from the MICU.Results: During PDSA cycle 1, 72 charts were randomly reviewed & 7 charts had a completed MERIT note (9.72% average). Thus far during PDSA cycle 2, 63 charts have been reviewed & 17 charts have completed MERIT notes (26.98%). Since implementation of relevant changes during PDSA cycle 2 there has been a steady increase in the completion rate of MERIT notes. Stakeholders were supportive & believe the initiative is successful at de-escalating medications & improving patient handoff.
Conclusions: Process changes led to an increase in the MERIT note completion rate, which has been positively received across stakeholders & reported improved patient handoff. Limitations include that completion rate is determined by random chart review & that de-escalation of these medications may occur without a completed MERIT note. Future directions will include additional PDSA cycles to further increase the MERIT note completion rate. There are ongoing efforts to analyze the prescribing rates of these medications on the discharge medication list of patients who had a MERIT note completed versus those that did not.