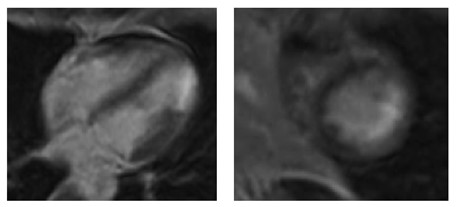
Case Presentation: A 48-year-old female presented with a 1-day history of exertional, non-positional, mid-sternal, severe chest pain associated with nausea, palpitations and dyspnea. She denied orthopnea, ankle swelling, cough, wheeze, coryza, fever, chills, or recent ill contacts. Past medical history: asthma, vertebral artery dissection, hypothyroidism, migraines, and severe acute respiratory syndrome coronavirus 2 (COVID-19) infection 4 months prior. No family history of cardiac disease. No smoking or illicit drug use. Medications: levothyroxine, albuterol inhaler and acetaminophen as needed. On arrival her pain was not alleviated by nitroglycerin or morphine. Vital signs and exam were unremarkable. EKG showed normal sinus rhythm with no ischemic changes; troponin was elevated at 1.10ng/mL. Chest x-ray was normal. Labs including renal function, inflammatory markers, coagulation panel, and d-dimer were within normal range. COVID-19 PCR testing was negative. She was given aspirin and high intensity statin.Due to persistent chest pain she underwent emergent left cardiac catheterization which showed nonobstructive coronaries and no evidence of spontaneous coronary artery dissection. She had recurrent chest pain the next day; troponin peaked at 14.2ng/mL. CT chest/abdomen with contrast showed no acute pathology. Echocardiogram demonstrated lateral/postero/infero–apical akinesis with left ventricular EF of 60%. Cardiac MRI showed normal biventricular size and systolic function and myocardial scar with focal wall motion abnormality in the apical lateral wall. Bisoprolol was added; she remained pain free. She was discharged on bisoprolol, statin, and aspirin.
Discussion: Cardiac injury in the setting of COVID-19 is widely varied and well established. The pathogenic mechanisms for cardiovascular involvement include direct viral damage, cytokine storm, oxygen supply-demand imbalance, inflammatory prothrombotic state, atherosclerotic plaque instability, hypoxic vasoconstriction and worsening of pre-existing conditions due to increase metabolic demand (1). It has clinically manifested in the form of viral and inflammatory myocarditis, type 1 and 2 myocardial infarction (MI), arrhythmias and heart failure exacerbation (1). These complications were largely found in patients infected with COVID-19 within 3 weeks of symptom onset (2,3). This case uniquely demonstrates myocardial infarction with nonobstructive coronary arteries (MINOCA) in a patient with remote history of COVID-19 infection. MINOCA has varied etiologies including myocarditis and thrombophilia (4) which are also associated with COVID-19 infection. This highlights the possibility of late cardiovascular complications following COVID-19.
Conclusions: This case uniquely demonstrates MINOCA in a patient with remote history of COVID-19. Awareness of possible late cardiovascular complications is critical for follow-up and warrants further investigation.