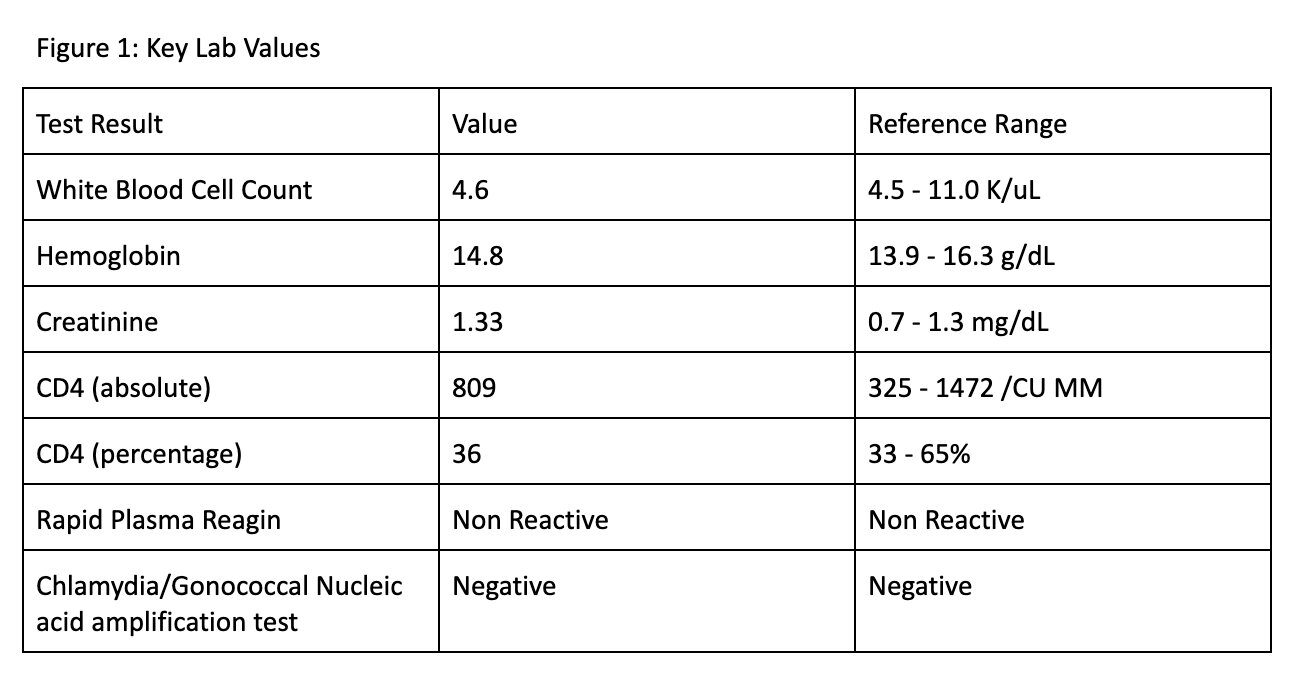
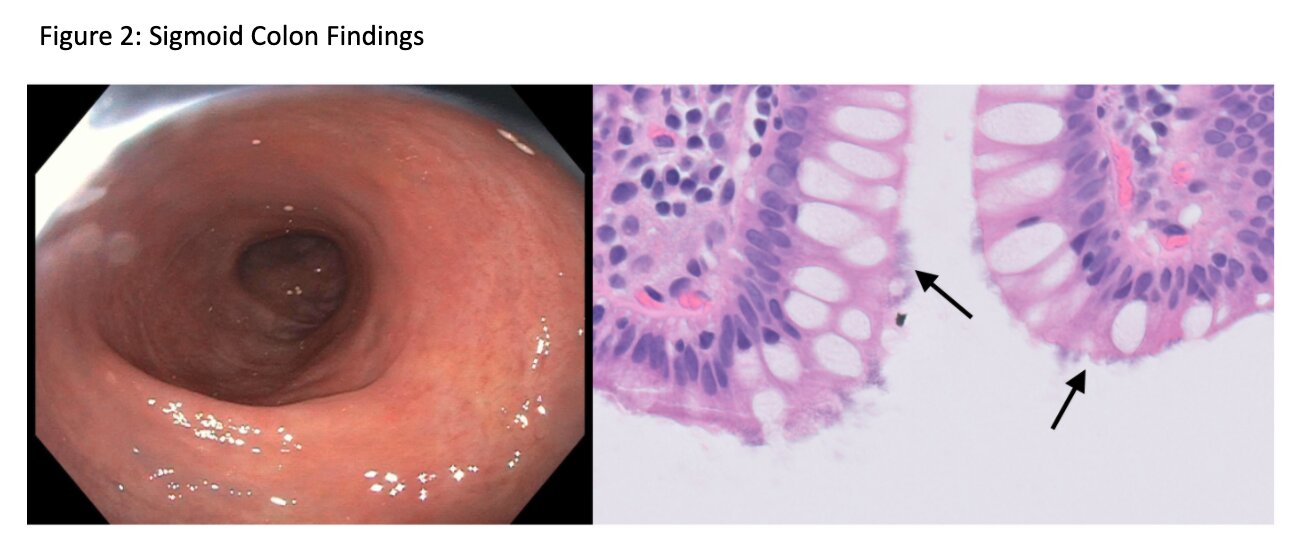
Case Presentation: A 40-year-old man with well controlled HIV and mild left-sided ulcerative colitis (UC) diagnosed 10 years earlier presented with several weeks of up to 10 watery stools per day with mild non-radiating crampy abdominal pain which improved after bowel movements. There was no hematochezia, tenesmus, weight loss, recent travel or sick contacts. His UC previously was treated with mesalamine, but he had been off this therapy for several years. Family history was notable for an uncle with UC. He was a social cannabinoid user and sexually active with male partners. Physical exam and labs were unremarkable, including a normal rapid plasma reagin and CD4 count (Fig 1). Colonoscopy revealed mild inflammation in the rectum and sigmoid colon, with a normal appearance of the rest of the colon. Biopsies from colonic segment revealed diffuse spirochetosis, with mild focal rectal cryptitis. The patient was treated with metronidazole 500 mg 3 times daily for two weeks, with complete symptom resolution.
Discussion: Human intestinal spirochetosis (HIS) is defined as the presence of anaerobic spirochetes on colonic epithelium. It can present with diarrhea, abdominal pain, gastrointestinal bleeding or often no symptoms at all. It is a rare condition with a reported incidence of only 0.7% in patients with chronic diarrhea, and most commonly affects HIV positive patients and men who have sex with men. Concurrent HIS in the setting of UC also is rare but has been infrequently reported. Although there are higher rates of HIS colonization in HIV-infected individuals, there is no correlation between degree of immunodeficiency and disease severity. This patient’s symptoms also could have resulted from a UC flare; however, the presence of only mild proctitis and the complete resolution of symptoms after taking antibiotics suggest that his symptoms primarily were due to HIS.
Conclusions: The patient’s history of both HIV and UC necessitated a broad differential diagnosis, as well as endoscopic and histologic examination, in order to make the correct diagnosis. This case demonstrates the importance of considering a rare infectious etiology such as HIS when initial testing does not identify a more common etiology for diarrhea.