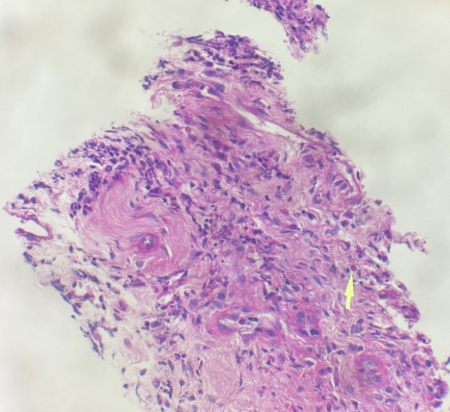
Case Presentation: 36-year-old male presented to ID clinic with painful left neck lump of 4 months duration worsening with pain and size for 2 months. Patient has h/o AIDS 2 years ago with cryptococcal meningitis, finished course of antibiotics and in remission with recent VL < 20, CD4 count 322, on daily Biktarvy. He also had syphilis treated successfully 2 yrs ago. PMH also includes Hypertension, ADHD and bipolar disorder with depression. On examination left supraclavicular swelling, tender with lymphadenopathy. Labs include WBC 8.61K, hemoglobin: 13.1, platelets 420 K, creatinine 1.3, AST: 37, ALP:97, ALT:35. Imaging studies show CT chest: Mass on superior mediastinum extending into left supraclavicular region, multiple pulmonary nodules and a node in lower left neck 2.5 x 1.8 cm. CT neck: Left supraclavicular lymphadenopathy and left superior mediastinal lymphadenopathy with areas of low attenuation and adjacent fat stranding, mildly enlarged left segment 2 lymph node measures 1.9 cm. Largest supraclavicular lymph node measures 2.6 x 1.9 x 2.1 cm Patient had undergone ultrasound guided FNA of left supraclavicular mass, pathology showed abscesses with Pneumocystis on GMS, negative for fungal, AFB or malignancy. He was treated with Bactrim DS q.8 hours for 6 weeks for neck abscess secondary to Pneumocystis. Bactrim was switched to atovaquone due to severe nausea. Repeat CT neck decreasing in size of the abscess.
Discussion: Pneumocystis carinii Pneumonia now named as Pneumocystis jirovecii Pneumonia is one of the fungal infection usually seen in immunocompromised individuals, HIV, malignancy, with altered immunity response. It is an ascomycetous fungus and diagnosis still remains challenging. In vitro Cultures of Pneumocystis jirovecii is not possible and diagnosis usually depends on the clinical, radiological and pathological staining. Incidence of PJP cases is down trending with use of prophylaxis. Pneumocystis jirovecii infection is commonly limited to lungs with 1-2.5% infections are extrapulmonary. It can involve spleen, lymph nodes, liver or bone marrow. Extra pulmonary symptoms are usually seen in severely compromised HIV patients with low CD4 counts and high viral loads. PCR (polymerase chain reaction) based diagnostic methods has high diagnostic yield. Other stains include Methanamine silver, giemsa stain are less sensitive.
Conclusions: There are very few case reports with skin involvement with pneumocystis. Skin disease can present as nodules, papules which can later ulcerate. Early diagnosis and treatment results in preventing severe complications. Treatment success rate is higher in HIV patients with early diagnosis and treatment. Prophylaxis is indicated in case of CD4 count less than 200 cells per millimeter. Patient who had PJP in the past will be on secondary prophylaxis. Primary or secondary prophylaxis should be discontinued in HIV patients if CD4 count continue to remain above 200 for a period of three months.