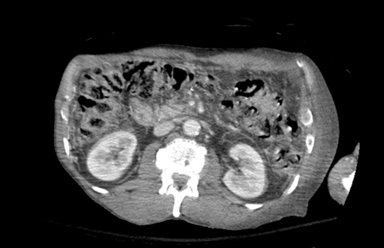
Case Presentation: The patient is a 64-year-old male with a history of decompensated liver cirrhosis due to alcohol use disorder, hepatic encephalopathy (HE) and duodenal mass status post Whipple procedure who presented with acute abdominal pain and confusion with erythema and drainage from the left side of his abdomen. Patient had a recent hospitalization for HE with ascites and spontaneous bacterial peritonitis and underwent multiple paracentesis, the most recent occurring 9 days prior to admission. Upon presentation, he was found to be in septic shock. On exam, he was alert and oriented only to self, with severe tenderness in the left upper and lower quadrants of the abdomen with associated crepitus, and purulent drainage. Ammonia and lactic acid levels were elevated. CT abdomen/pelvis with contrast revealed diffuse anasarca with severe foci of the anterior abdominal wall concerning for necrotizing fasciitis (NF) (Figure 1). CT head without contrast showed no acute findings. He was admitted to the ICU. IV cefepime, vancomycin and clindamycin were started. Rifaximin and lactulose were initiated for hepatic encephalopathy. The patient was evaluated by general surgery and underwent urgent abdominal wall debridement. He remained intubated and sedated postoperatively. Blood cultures from a recent admission were positive for multidrug resistant Klebsiella pneumonia that was thought to be falsely sensitive to ceftriaxone, as the organism demonstrated resistance to several other antibiotics. Therefore, meropenem was initiated, and cefepime was discontinued, with continuation of vancomycin and clindamycin. Ammonia and lactate levels normalized, and he was extubated as mentation improved. He was not a candidate for transplant after clinical improvement due to his ongoing alcohol use.
Discussion: Abdominal paracentesis is a safe, minimally invasive procedure, with complications such as hemorrhage, perforation, or infection being rare with proper technique [1]. Abdominal wall NF following recent paracentesis is uncommon and not well described in literature. It is a rare soft tissue infection, causing rapid necrosis of the fascia and subcutaneous tissue. The perineal region, Fournier’s gangrene, and lower extremities are most often affected [2]. Reported risk factors including trauma wounds, health-care-related wounds, insect bites, with diabetes mellitus being the most common [3]. Patients with grade C cirrhosis and diabetes mellitus are associated with increased mortality with NF, as hepatic decompensation exacerbates infection severity [4]. Early detection of abdominal wall NF is essential for preventing further complications. Clinical presentation may resemble cellulitis or abscess, delaying intervention. Severe pain disproportional to exam, erythema and edema should raise suspicion for NF. CT imaging can support diagnosis showing subcutaneous gas or focal changes. Urgent surgical debridement is the mainstay of treatment and delay increases mortality [3]. Early administration of broad-spectrum antibiotics is also critical.
Conclusions: Abdominal wall NF is a rare, life-threatening soft tissue infection. Abdominal wall NF after paracentesis is not well described in literature. This case emphasizes the importance of prompt recognition, early initiation of broad spectrum antibiotics and emergent surgical debridement. Clinicians should maintain a high index of suspicion for this infection in patients with cirrhosis, even after minor procedures such as paracentesis.