Background: In utero opioid exposure can result in neonatal abstinence syndrome (NAS). NAS incidence has increased five-fold in the last decade. NAS is a serious condition characterized by central nervous system hyperirritability and autonomic nervous system and gastrointestinal tract dysfunction. Newborns with NAS may have several potential complications, may require pharmacological management, have increased hospital costs, and have a prolonged hospital length of stay (LOS). Opioid use disorder in pregnant women and NAS are now considered a public health crisis.
Several non-pharmacologic interventions may assist in the care of NAS. One of these interventions include a parent or guardian rooming in with the infant in which the patient has a private room and the parent(s) or guardian provide care and holding in addition to the nursing staff. The parent or guardian may also sleep in the same room. In tertiary care settings, rooming in has been demonstrated to decrease LOS, cost of care, and medication required to treat NAS.
Methods: Intervention 1:
At the community site, initially standard of care for a newborn with NAS was to admit to a Neonatal Intensive Care Unit (NICU) for management and discharge to home from the NICU when stable and no longer requiring medications. The level 2 NICU at the community study hospital did not have rooming in capability for the parents. With the intervention, newborns were transferred from the NICU to the inpatient pediatric ward when stable and weaning from medications. The pediatric ward has the capability for a parent or guardian to stay in a single room with the newborn for up to 24 hours a day.
Ongoing interventions:
Based on the success of rooming in at this hospital, the inclusion of families in care was incorporated into the comprehensive NAS program. The program has goals and implementation strategies that include:
Standardizing policies
Standardizing pharmacologic and non-pharmacologic practice guidelines
Staff and referring partner education
Family education
Staff and family engagement
Expanding cuddler availability
Lactation support and breastfeeding education
Real time program review of individual patients
Creating a care coordinator position to follow patients through the hospital stay
Creating a developmentally appropriate environment for newborns with NAS
Novel strategies to coordinate this program and offer direct patient interventions include having a social worker care coordinator and pediatrician review all inpatient cases frequently during the admission to assess care barriers and to offer guidance for optimal care management.
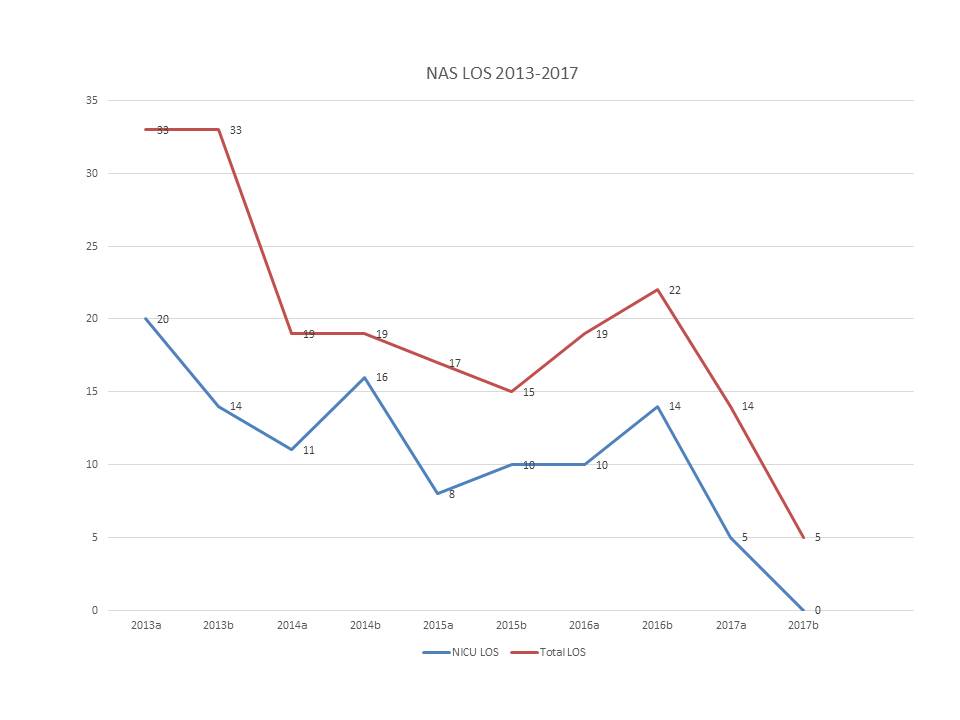
Results: Over a 4 year study period, LOS in the NICU decreased from 20 days on average to 5 days (75% reduction). Total hospital LOS decreased from 33 days to 12 days (64% reduction). (See also graph.) There were no differences between groups in complication rates or readmissions.
Total cost of care per episode decreased 30% from 2016 to 2017. Breast-feeding rates increased 70% from 2016 to 2017. Over 80% of eligible patients are breast-feeding exclusively or using combination breastmilk and formula feedings. Medication usage for NAS declined over one third from 2016 to 2017.
Conclusions: This implementation of rooming in demonstrates that rooming in can be done safely and effectively at community hospitals. Rooming in may become standard of care for NAS if the capability exists at a facility.
A comprehensive care model and use of population health strategies can be applied to neonatal medical conditions with success.