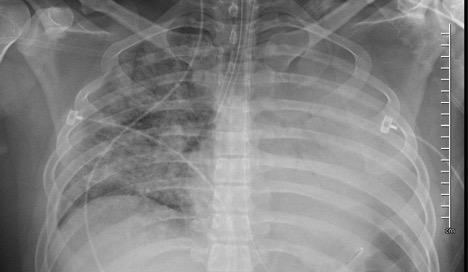
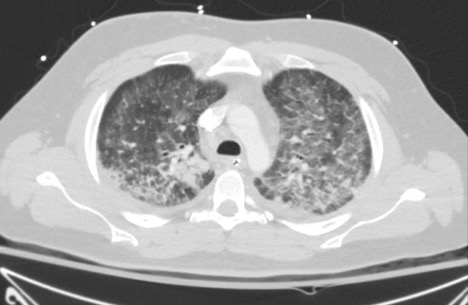
Case Presentation: 22-year-old Caucasian male who presented to our Texas hospital with dyspnea. His symptoms started two days prior with fever to 103°F, vomiting, and a cough with white sputum. The patient worked as a bartender and endorsed daily tetrahydrocannabinol (THC) vaper use. Upon admission, he exhibited tachycardia (137 bpm), tachypnea (30 bpm), hypoxemia (O2 saturation 80%), hypotension (75/55), and use of accessory muscles. The patient was intubated for hypoxemic respiratory failure and started on mechanical ventilation. Initial laboratory workup revealed a pro-calcitonin of 0.92 ng/mL without leukocytosis. Urine drug screen was positive for marijuana. Chest x-ray demonstrated findings consistent with pneumonitis. Chest CT demonstrated diffuse ground-glass infiltrates. Bronchoscopy with bronchoalveolar lavage revealed reactive cells. Autoimmune, viral, and parasitic etiologies were ruled out. Given the patient’s findings, empiric coverage for pneumonia and steroids for pneumonitis were initiated. However, the patient’s condition continued to deteriorate with a PaO2/FiO2 ratio of 109 despite high ventilator settings and broad spectrum antibiotics. Thus, our team began to suspect atypical chemical pneumonitis secondary to vaping and EVALI was diagnosed. We continued steroids for 7-days and the patient was successfully extubated. Upon discharge, initial imaging abnormalities were completely resolved. The patient endorsed complete resolution of his dyspnea at his one-month follow-up appointment.
Discussion: E-cigarette, or vaping, product use associated lung injury or EVALI is a new pathology, described by the CDC as idiopathic damage of vaping products to the lungs. Emerging data aims to elicit the pathophysiology behind EVALI. Currently, there are no clinical practice guidelines for EVALI and empiric therapies have not demonstrated clear success (1). We describe the diagnosis and treatment of a 22-year-old male with EVALI. The use of e-cigarettes and vaping has increased tremendously in the last 2-3 years. High school students are the highest consumer population, with 27.5% endorsing e-cigarette in the past 30 days (2). Among teen e-cigarette users, only 13.2% are aware that e-cigarettes contain nicotine (3). 40% of e-cigarette users aged 18-24 years have never been regular cigarette smokers (2). The pathophysiology behind EVALI is controversial. Preliminary studies suggested that EVALI is related to vitamin E evaporation provoked by vaping devices. Vitamin E acetate is used as a diluent in 48% of THC vaping products (4). Initial studies proposed that evaporated vitamin E is absorbed by macrophages then consolidated, causing lipoid pneumonia. However, recent findings described by Larsen et. al. show histopathological findings consistent with acute lung injury, including acute fibrinous pneumonitis, diffuse alveolar damage, or organizing pneumonia (1). These findings suggest that EVALI is more likely to be a form of airway-centered chemical pneumonitis secondary to inhaled toxic substances, versus exogenous lipoid pneumonia.
Conclusions: This case demonstrates the growing importance of recognizing EVALI. The diagnosis and treatment of EVALI continues to be challenging given the absence of clinical practice guidelines for this novel pathology; however, the current cornerstones of treatment are airway maintenance, symptom management, and steroid-use. Physicians should also educate their patients about the potential dangers of e-cigarettes and vaping products.