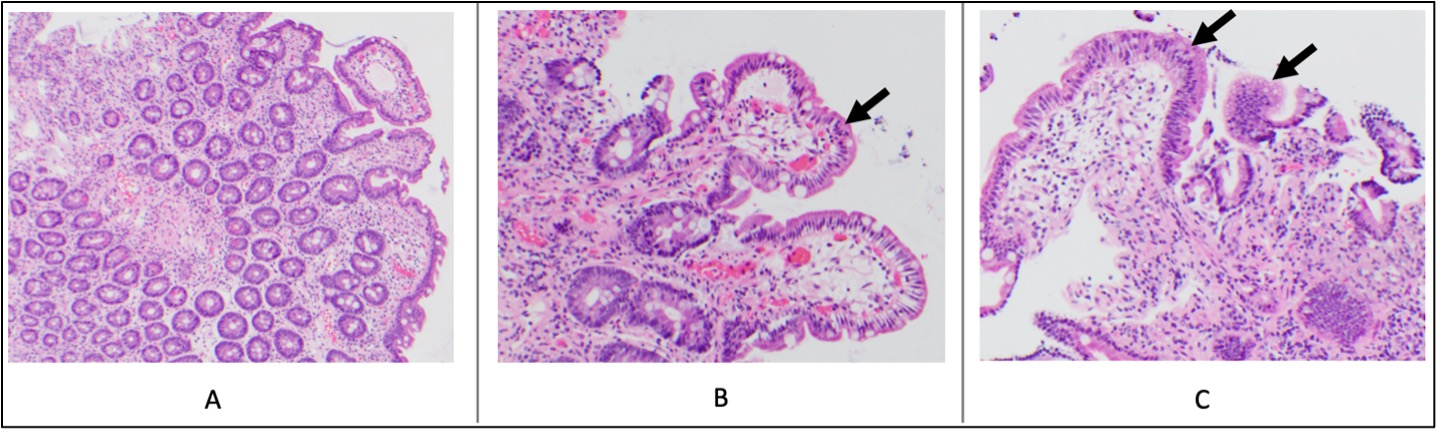
Case Presentation: A 66-year-old female with pan-hypogammaglobulinemia from therapies for stage IV diffuse large B-cell lymphoma (DLBCL) and psoriatic arthritis on aprimelast presented with 6 months of severe diarrhea and hypokalemia. She achieved complete remission of DLBCL with R-CHOP and CAR-T therapy 15 and 8 months before symptom onset, respectively. Severe pan-hypogammaglobulinemia was detected 3 months prior to symptoms.She developed watery, non-bloody, non-mucoid diarrhea 6 months before presentation, experiencing up to 30 episodes daily. After 3 months of symptoms, she sought evaluation. Labs showed hypokalemia (1.9 mmol/L; reference range [RR] 3.4-4.8 mmol/L), leading to hospitalization. Diagnostics revealed stool osmotic gap consistent with secretory diarrhea; gastrointestinal pathogen panel (GIPP) positive for norovirus; negative stool Clostridium difficile assay, ova and parasite panel, calprotectin, adenovirus, and CMV PCR; negative serum anti-tissue transglutaminase, celiac disease associated HLA alleles DQ2 / DQ8, and HIV antigen/antibody; normal serum thyroid stimulating hormone; low serum IgG (147 mg/dL; RR 646-2013 mg/dL), IgM (< 8 mg/dL; RR 40-230 mg/dl), IgA (< 15 mg/dL; RR 70-400 mg/dL), and IgE (< 2 IU/mL; RR 2-214 IU/mL). Colonoscopy revealed pan-colonic congested mucosa with minimal microscopic neutrophilic colitis. Esophagogastroduodenoscopy was grossly normal; duodenal biopsies showed patchy mild-to-moderate villous blunting, focal foveolar metaplasia, and minimally increased intraepithelial lymphocytes (Figure 1). Intravenous immunoglobulin (IVIG) improved symptoms for one day, but they returned, prompting a 5-days of nitazoxanide with colestipol, potassium supplementation, and anti-diarrheals. She improved and discharged with potassium supplementation. One month later, she was re-admitted with hypokalemia and worsened diarrhea. Labs showed pan-hypogammaglobulinemia and a GIPP positive for norovirusShe was diagnosed with chronic norovirus infection. Treatment included IVIG, nitazoxanide, and anti-diarrheal. With ongoing symptoms, enteral immunoglobulin was initiated. Diarrhea slowed and potassium normalized by discharge. One year later, she continues with biweekly IVIG infusions.
Discussion: Noroviruses are non-enveloped, single-stranded RNA viruses from the Caliciviridae family and are the leading cause of acute gastroenteritis. They spread via fecal-oral routes, contaminated food and water, airborne droplets, and fomites. In immunocompetent individuals, symptoms are usually mild and self-limiting (vomiting, nausea, watery diarrhea). However, in immunocompromised patients, norovirus can cause severe, prolonged symptoms, increasing morbidity, mortality, malnutrition, and intestinal barrier dysfunction.1-5 This case is the first to document villous blunting in a patient with lymphoma-related immunosuppression.6Chronic norovirus treatment varies in success. Ribavirin has worked for some but faces resistance in common variable immunodeficiency.7-6 Enteral immunoglobulin has improved symptoms but does not significantly reduce resolution time or hospitalization costs.10 Nitazoxanide’s effectiveness ranges from no improvement to complete resolution.11,12
Conclusions: This case highlights the rarity and significance of chronic norovirus in immunocompromised patients, emphasizing management challenges and the need for careful diagnosis and tailored therapies.