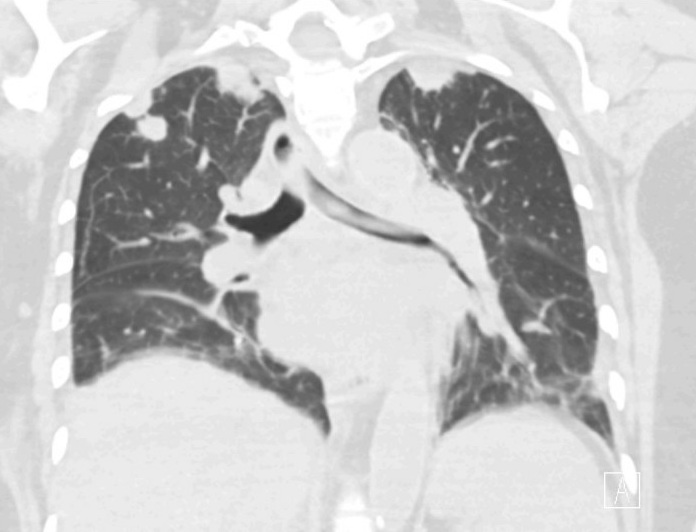
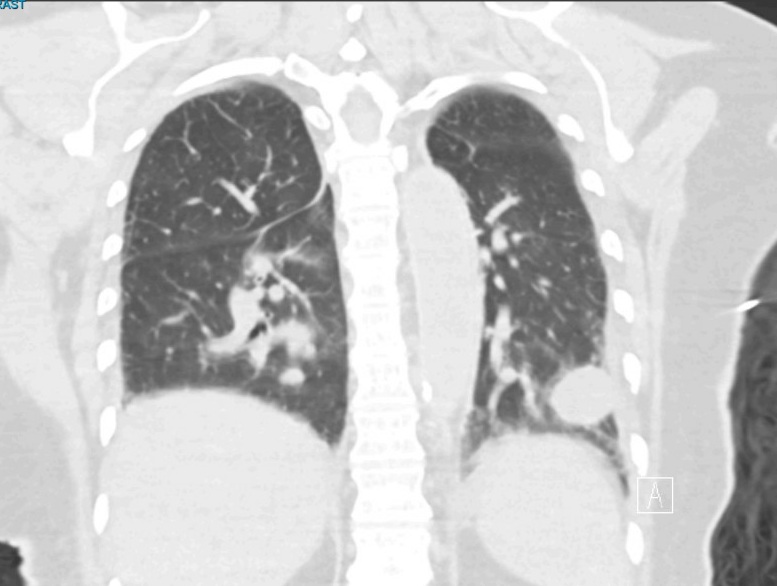
Case Presentation: A 75-year-old woman with depression, anxiety, and bilateral hearing loss presented after syncope and was admitted for new-onset atrial fibrillation and new bilateral lung nodules. She reported intermittent chest tightness and 2 weeks of progressive exertional dyspnea. She also noted decreased appetite and severe night sweats.Over the preceding year, she developed profound bilateral hearing loss and ear discomfort. Her otolaryngologist ordered a CT scan that showed bilateral otitis media and acute sinusitis which did not respond to multiple courses of treatment. Recent age appropriate cancer screening was negative. She reported a remote 20 pack-year smoking history. She had no known tuberculosis risk factors. Family history was notable for “throat cancer” in her brother. On exam, the patient was afebrile, hemodynamically stable, and oxygenating well on room air. She was tachycardic with irregular rhythm. Bibasilar rales and conductive hearing loss were observed, but otherwise her exam was unremarkable.Emergency department evaluation showed: mild leukocytosis with neutrophilic predominance and normal eosinophils. BMP and hepatic function panel were unremarkable. Non-contrast chest CT showed multiple bilateral pulmonary nodules (Figure 1), some cavitary, with a dominant left lower lobe lesion (Figure 2), read as most consistent with metastatic disease.During hospitalization, workup for infectious causes of cavitary lung lesions was negative. ESR and CRP were markedly elevated, and pleural fluid cytology was negative for malignancy. Rheumatologic testing showed weakly positive c-ANCA and markedly elevated PR3 antibody. After infection was excluded, prednisone 60 mg daily was started. Urine evaluation showed no dysmorphic red blood cells, so renal biopsy was considered low yield. VATS lung biopsy demonstrated necrotizing granulomatous inflammation, confirming granulomatosis with polyangiitis.
Discussion: Granulomatosis with polyangiitis (GPA) is an ANCA‑associated small‑vessel vasculitis characterized by necrotizing granulomatous inflammation, classically affecting the upper airways, lungs, and kidneys. ENT‑predominant disease—chronic “sinusitis,” otitis media, and progressive hearing loss—is common and often precedes systemic involvement by months to years. These presentations are frequently misattributed to recurrent infection or eustachian tube dysfunction, leading to repeated antibiotics and steroids rather than vasculitis evaluation. Diagnostic delay increases the risk of irreversible organ damage, including permanent hearing loss, renal impairment, and destructive sinonasal disease. In this patient, a year of refractory otologic and sinus symptoms, followed by constitutional features which should have led to a workup for GPA, but unfortunately focus remained anchored on primary ENT pathology.
Conclusions: This case highlights how failure to recognize ENT‑predominant GPA can delay diagnosis and treatment. In patients with refractory sinus or ear disease plus systemic or pulmonary findings, early ANCA testing and rheumatology referral should be considered. Prompt recognition of GPA allows timely initiation of immunosuppression, reducing the risk of irreversible hearing loss, pulmonary destruction, and renal failure.