Background: Heart failure (HF) is a common, chronic clinical syndrome often accompanied by episodes of acute decompensation driven by volume overload (1). Reversing this overloaded state is the principal goal in treatment of acute decompensated HF, typically achieved using loop diuretics (2). Despite ubiquitous use of loop diuretics, guidance on initial dosing strategies remains limited (3-5). We hypothesized that an optimal dose based on the relationship between inpatient-to-home diuretic (I2H) ratio would result in lower lengths of stay (LOS) when given early in hospitalization.
Methods: We conducted a retrospective study of adult patients hospitalized with HF exacerbation at a large academic hospital from years 2014 to 2018. Demographic and clinical data were abstracted from electronic health records, and patients with end-stage renal disease (ESRD) were excluded. The I2H ratio was calculated by dividing the diuretic dose given within the first 24 hours of hospitalization by the daily home dose of diuretics. All diuretics doses were converted to furosemide equivalents. The I2H ratio was then categorized into three categories: ≤1.5, 1.51 to 3, and >3. Data were summarized using mean (SD), median (IQR) as appropriate for continuous variables and as frequencies with percentages for the categorical variables. Relationship between LOS and I2H ratio categories was determined using unadjusted and adjusted generalized linear models (GLM) with log-link and gamma distribution to account for the right-skew of the LOS. Models were adjusted for age, gender, race, BMI, case-mix index (CMI), Charlson comorbidity Index (CCI), serum creatinine, hemoglobin, presence of diabetes, hypertension, or chronic kidney disease, and whether patients were in an intensive care unit (ICU) during hospitalization. Model fit was determined by examination of deviance residual diagnostics. A p-value<0.05 was considered significant.
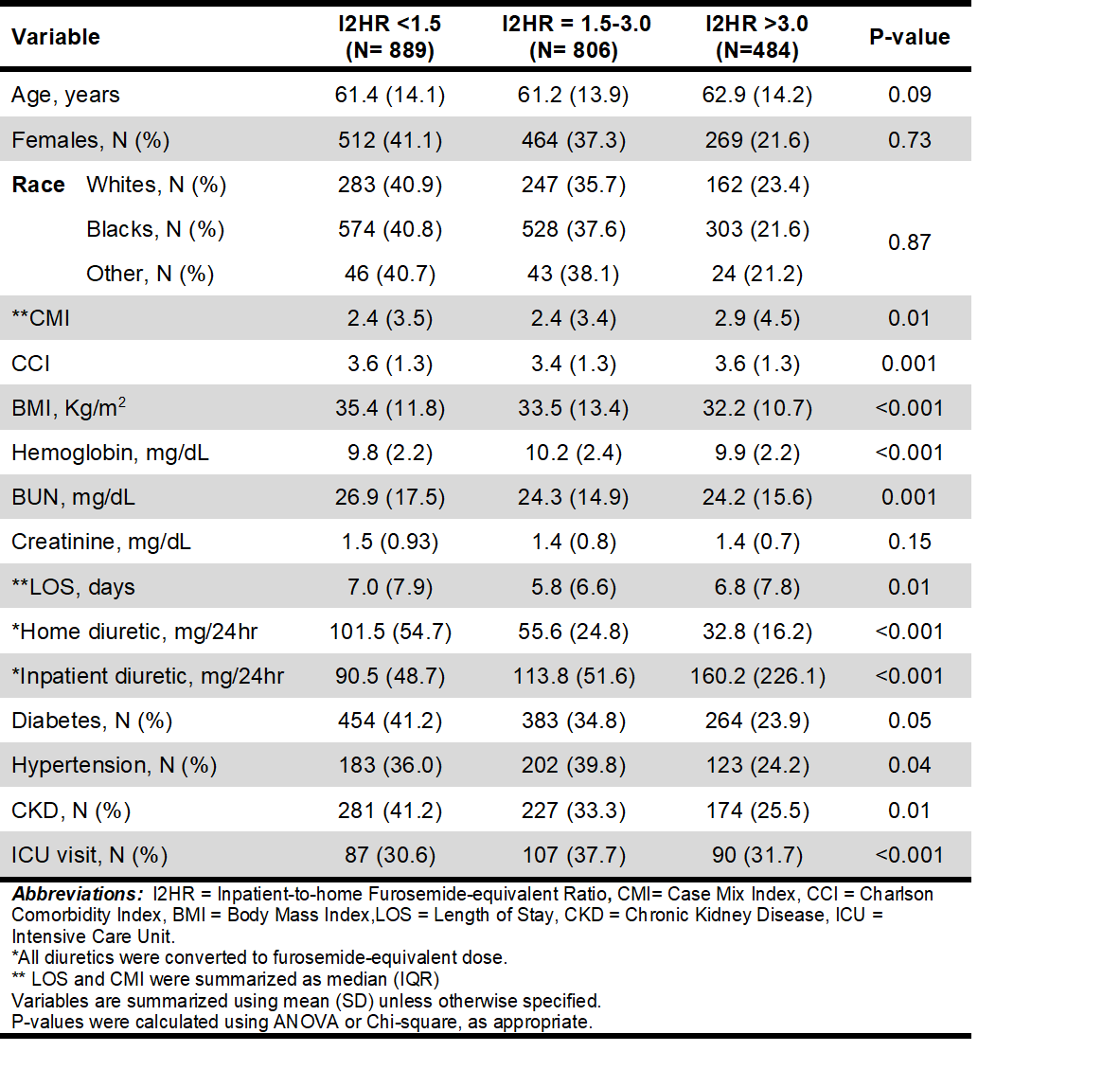
Results: Of the 2,179 hospital admissions, 1,245 (57%) were females, 1,405 (63%) were African-Americans, 1,101 (50.5%) had diabetes, 508 (23.3%) had hypertension, and 284 (13%) spent at least some time in an ICU. Mean (SD) age was 61.7 (14) years, BMI 34 (12) Kg/m2, and CCI 3.5 (1.3). Median (IQR) LOS was 6.6 (7.7) days, CMI 1.5 (1.0), and I2H ratio was 2 (1.5). Patients in the three categories of I2H ratio differed in several aspects (Table). LOS was significantly lower in the group with I2H ratio 1.5-3.0 than the other two groups. In the unadjusted model, patients with I2H ratio 1.5-3.0 had 11% lower LOS (difference= -11%, 95%CI= -18%, -5%; P=0.001) while those with I2H ratio >3.0 had no difference (difference=-3%, 95%CI= -10%, 5%; p=0.51) from patients with I2H ratio <1.5. The results did not change in adjusted models – patients with I2H ratio 1.5-3.0 had 8% lower LOS than patients with I2H ratio <1.5 (difference = -8%, 95%CI = -14%, -3%; P=0.005) and there was no difference between patients who had I2H ratio <1.5 and those with I2H ratio >3.0 (difference = -6%, 95%CI = -12%, 1%; P=0.09)
Conclusions: Among adults hospitalized with acute HF exacerbation, an I2H ratio of 1.5-3.0 was associated with the lowest LOS. Clinicians can use this data to help guide initial dosing of diuretics for patients presenting with acute HF exacerbation.