Outcomes of an ‘Attending-Only’ Hospitalist Bedside Procedure Service
Background: Patients admitted to the hospital frequently require bedside procedures including central venous catheter placement, paracentesis, thoracentesis, and lumbar puncture. Procedure training varies across residency programs resulting in varying levels of competency among practicing physicians.1 In addition, the time consuming nature of these procedures has led to a decrease in procedures performed by internists at the bedside and an increase in outsourcing to interventional radiologists.2 which can in turn further decrease procedural competence and increase delays in time to procedures. In response, many academic medical centers have developed dedicated procedure services involving residents to improve both care and education3, however, this intervention would not benefit hospitals who do not have access to trainees. We created a procedure service within an academic medical center not staffed with residents or trainees, to determine the potential impact of a hospitalist attending run procedure service on a hospital system.
Objective:To determine the impact of an attending-only hospitalist run procedure consultation service on complication rates, time to procedure, and revenue generation.
Methods: Eight hospitalists at a tertiary care academic medical center completed standardized ultrasound guided bedside procedure training for central venous catheter placement, paracentesis, thoracentesis, and lumbar puncture. One nurse clinician assisted with accepting consults, procedure set up, follow up and data collection. One trained hospitalist and the nurse clinician were assigned to the procedure service from August 2014 through October 2015. For each procedure administrative, clinical, and financial data were collected including: consulting service, patient and clinical characteristics, procedure type, procedure outcomes, complications, and charges.
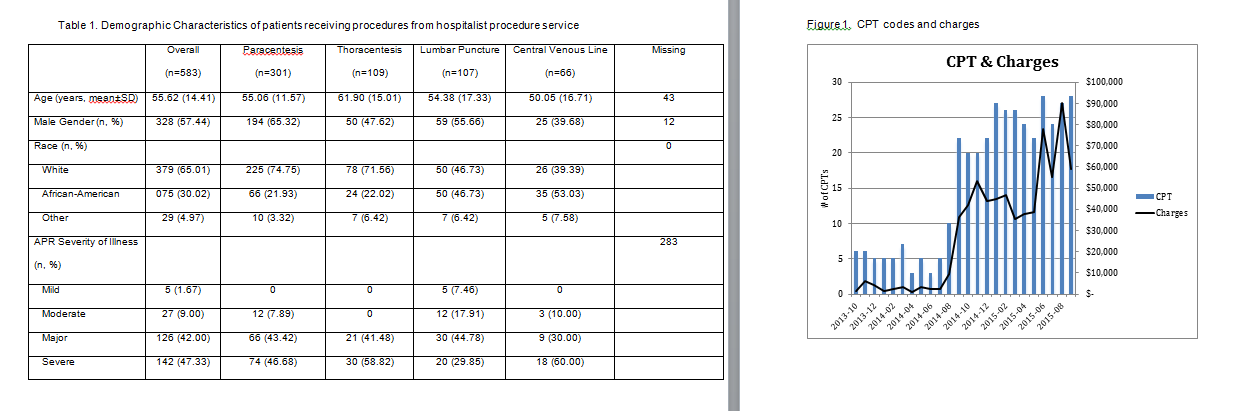
Results: Between August 2014 and November 2015 there were a total of 586 consults to perform bedside procedures, of which 546 (93%) were attempted. Of the procedures attempted 499 (91%) were successful. There was one procedure related complication (0.18%) and the average time from consult to procedure completion was 0.01 days. The total number of procedure CPT codes and charges billed for the hospitalist program increased from an average of 5.1 CPT codes per month ($2707.70 billed per month) in the year prior to the start of the procedure service to 23.3 CPT codes per month ($47,972 billed per month) after the procedure services’ inception.
Conclusions: A bedside procedure service staffed by hospitalists can yield low wait times for procedures without increasing complication rates and can simultaneously increase revenue. An ‘attending-only’ staffed procedure service model is feasible and may have broader implications for other Hospitalist programs in settings other than academic medical centers.