Background: Throughout the COVID-19 pandemic, clinicians have sought to identify risk factors for severe disease to help guide hospital algorithms, resource allocation and therapeutics. Older age, high Charlson Comorbidity Index (CCI), D-dimer and C-reactive protein (CRP) are associated with severe disease (1-5). CCI and SaO2/FiO2 ratio are associated with mortality, but the changing SaO2 in time makes it difficult for clinicians to use as a predictor of disease severity (6). We sought to find objective markers upon hospital presentation to predict COVID-19 outcomes in Veterans.
Methods: This is a retrospective, single center study of Veterans hospitalized from 3/18/20 to 7/13/20 with COVID-19 diagnosed by PCR. Demographic, clinical and laboratory variables were queried for association with supplemental O2 requirement within 24 hours of admission (AdmO2), peak disease severity (PDS) and outcomes. PDS was divided into 3 categories based on O2 need during hospital stay: Mild (0-3L/min by nasal cannula (NC)), Moderate (4-6L/min NC or nonrebreather mask), and Severe (O2 via high flow NC, non-invasive positive pressure ventilation (NIPPV) and/or mechanical ventilation). We used STATA/IC v16 for statistical analysis. Two-sample T test and ANOVA compared continuous variables between two groups or more. P-values for categorical variables correspond to Pearson’s χ^2 tests. Linear, logistic, and ordered logistic regression models were used to identify predictors for the studied outcomes.
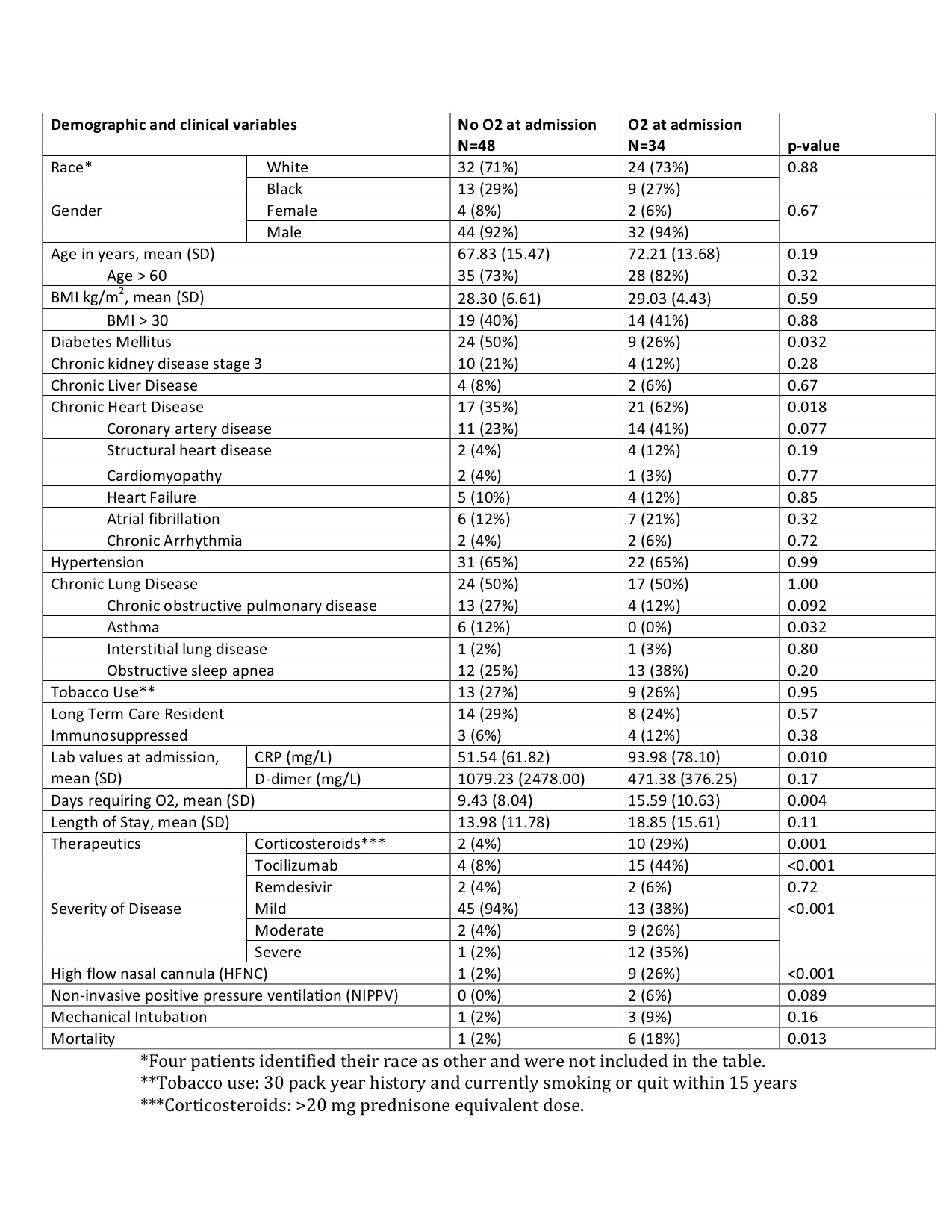
Results: Of the 85 COVID-19 inpatients during the study period, 82 were included in final analysis (3 spent several days at other hospitals before admission). Mean age was 69.7 years (SD 14.8), majority being men (N=76), 68.3% White, 26.8% Black and 27% were active smokers. Commonest comorbidities were hypertension (65%), chronic lung disease (50%) and chronic heart disease (CHD) (46.3%). Mean BMI was 28.4 (SD 5.1). Table 1 outlines patient characteristics and outcomes stratified by AdmO2. 34 patients (41%) needed AdmO2 and 48 (59%) did not. Age, race, gender and BMI were not associated with AdmO2. CHD was a risk factor for AdmO2 (p = 0.018). There was no correlation between days of symptoms prior to presentation and AdmO2 (p = 0.802). Mean CRP at admission was higher in AdmO2 group (p = 0.01) while D-dimer did not vary between groups (p = .17). The AdmO2 group required O2 for more days (15.59 vs 9.43, p =0.004). There was no difference between length of stay in both groups (p = 0.06). AdmO2 received more therapeutics and NIPPV (p <0.001) but there was no difference in mechanical ventilation (p = 0.16). There was more severe disease in the AdmO2 group (p = <0.001). The odds of progressing from mild disease to moderate and from moderate disease to severe were 3.19 times higher in the AdmO2 group (95% 1.84 to 4.55, p <0.001) . AdmO2 was also a risk factor for mortality (p = 0.013).
Conclusions: Our study identified oxygen requirement within 24 hours of admission as a predictor of disease severity, progression of disease, number of days on O2 and mortality. AdmO2 can therefore be a helpful prognostic indicator in hospitalized COVID-19 patients and can help with resource allocation, early triaging and timely management. Larger and more focused studies are needed to determine how therapeutics can impact the trajectory of illness in these patients. Of note, duration of symptoms before admission did not impact AdmO2.