Background: Medical training relies on direct observations and formative feedback. After graduation, opportunities to receive feedback on clinical teaching diminish. Hospitalists typically receive feedback through learner evaluations which can be untimely, non-specific, and biased. The objective of this study was to examine if feedback after peer observation results in improved inpatient teaching behaviors.
Methods: Academic hospitalists observed their peers during bedside teaching rounds, using a standardized tool based on the Stanford Faculty Development Program. The tool focused on five of the teaching domains (learning climate, control of session, promotion of understanding and retention, evaluation, and feedback) based on relevance to the inpatient environment. Hospitalists were observed at the beginning and end of their rotation to allow for incorporation of the feedback. A post-observation survey assessed the hospitalists’ and observers’ comfort level with observation and the utility of the feedback.
We used mixed models with crossed design to account for correlations between the observations. We adjusted all models for gender, age, and years of experience. We tested the internal validity of the instrument with Cronbach’s alpha.
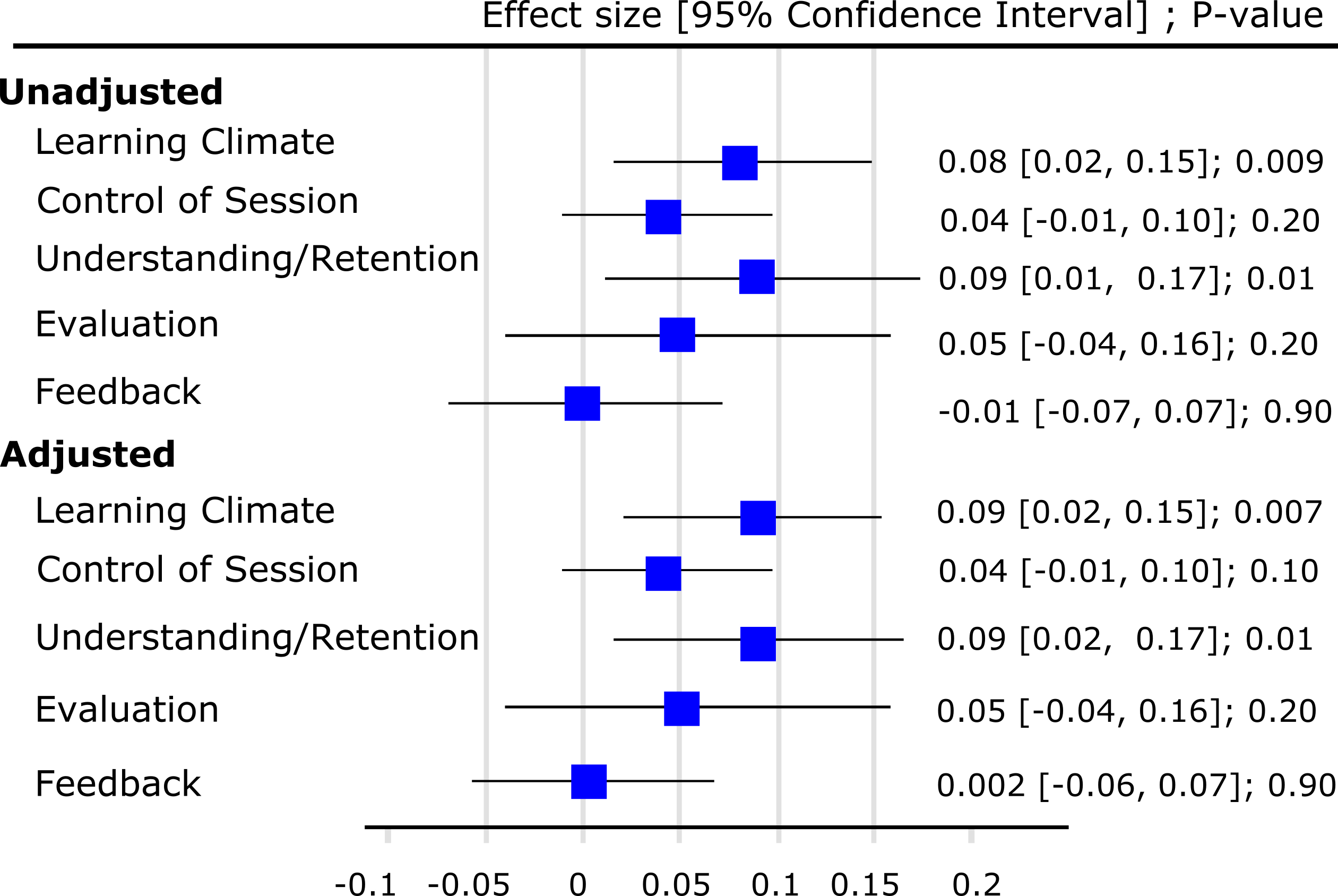
Results: Seventy observations were performed involving 27 hospitalists. Hospitalist age was 37.5±4.9 years with experience of 6.4±4.2 years. Majority were females (70.4%), Caucasian (67%), and graduates of United States medical schools (85.2%). Sixty-four percent reported being “very comfortable” with the observation, 53% found the feedback “very helpful,” and 89% were comfortable with future observations. All observers felt the tool was easy to complete, and 88% found the observation to be helpful for their own teaching. Correlation between any two teaching domains ranged from 0.3 to 0.7 (all p-values < 0.05) with Cronbach’s alpha of 0.81. In unadjusted and adjusted analysis, mean improvement in teaching behaviors with each observation was associated with increased scores in two domains, learning climate and promotion of understanding and retention (Figure 1).
Conclusions: Peer observation and feedback resulted in a significantly positive improvement in two teaching domains. The hospitalists involved found the experience valuable. At the teacher level, direct observation using a standardized tool provided immediate feedback of desired teaching behaviors, leading to their timely adoption. Peer observations created a shared mental model of good clinical teaching. As we saw positive results in less than a year of observations, our process may allow for rapid, consistent development of faculty.