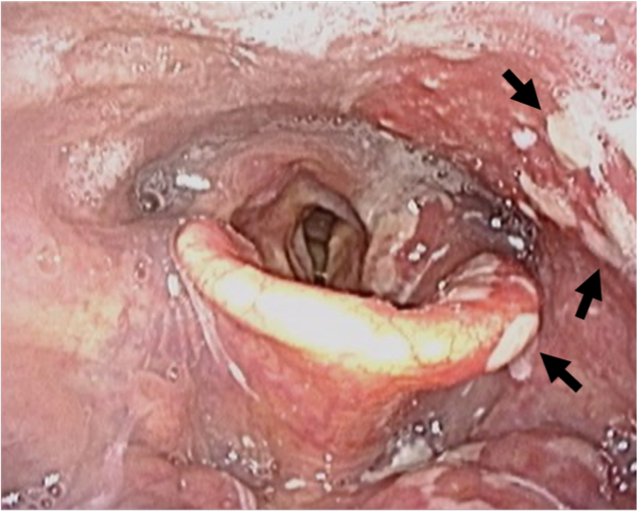
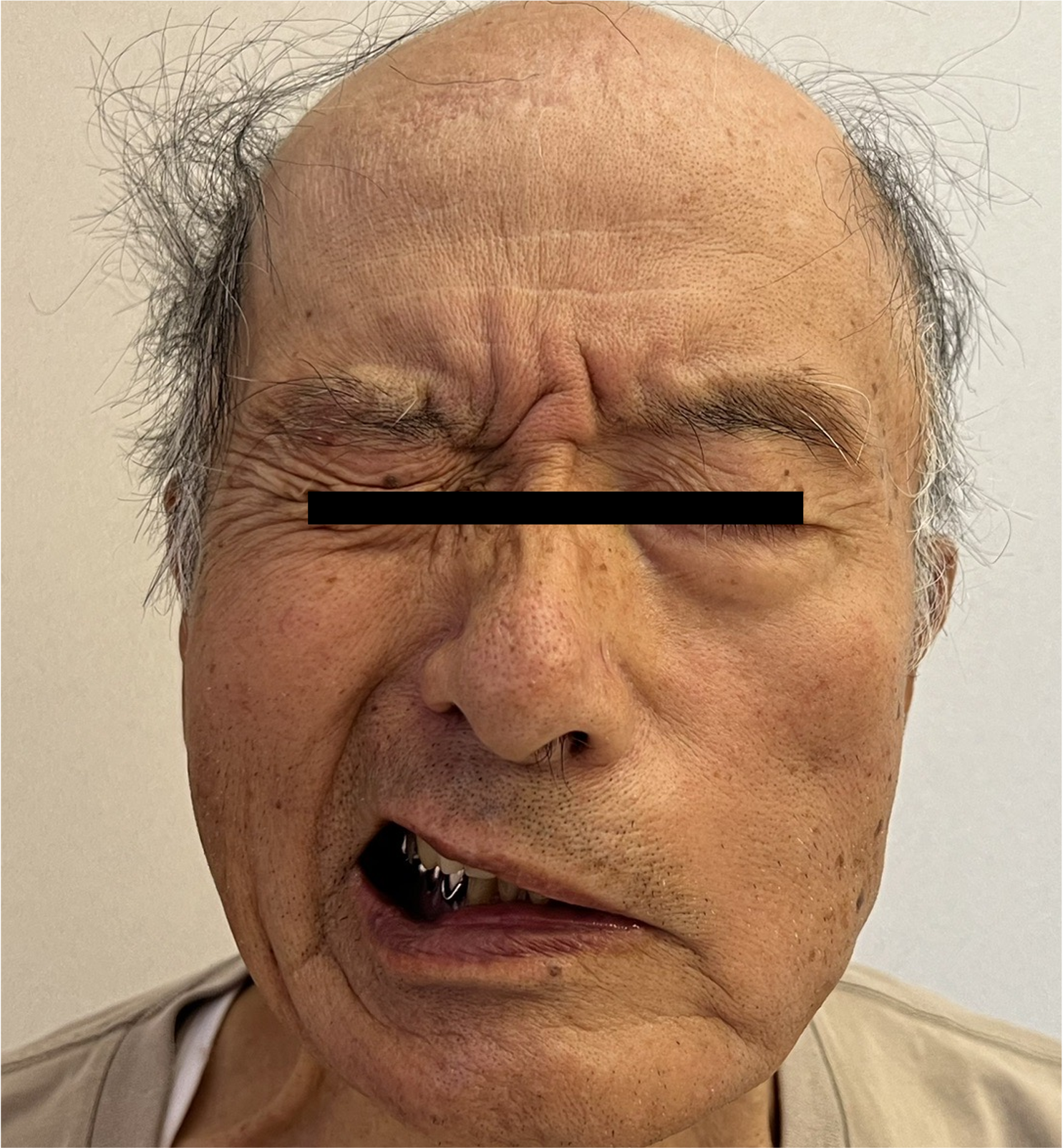
Case Presentation: An 83-year-old Japanese man with hypertension presented with painful oral ulcers localized to the left side. He later developed a sore throat, dysphagia, and hoarseness, prompting admission. He was referred to the otolaryngology department, where laryngoscopy revealed ulcers confined to the left oropharynx and partial paralysis of the left vocal cord (Fig. 1). Varicella-zoster virus (VZV) reactivation was suspected, and oral valacyclovir was initiated.On day 5, he developed sharp, shock-like neuropathic pain involving the left parietal region, left forehead, preauricular area, and lower jaw, distributed in an “onion-skin pattern.” On day 8, he experienced three episodes of syncope upon standing. Orthostatic testing revealed a marked drop in BP from 101/65 mmHg (HR 51/min) in the supine position to 67/42 mmHg (HR 48/min) after 2 minutes of standing, indicating severe autonomic dysfunction. On day 15, new left-sided facial nerve palsy was observed (Fig. 2). Serology was positive for both VZV IgG and IgM, consistent with VZV reactivation involving multiple cranial nerves (V, VII, IX, and X). CSF showed mild mononuclear pleocytosis (13 cells/μL), while VZV DNA was not detected by PCR. Brain MRI and CT imaging of the chest and abdomen revealed no tumor or other structural abnormalities. These findings confirmed VZV reactivation.High-dose prednisolone (60 mg/day) was initiated, resulting in rapid improvement in facial palsy, neuropathic pain, and orthostatic hypotension. Steroids were tapered over one month. At 3-month follow-up, all neurological symptoms had completely resolved.
Discussion: While VZV classically reactivates in dermatomal distributions, it can also cause multiple cranial neuropathies. This patient’s sequential involvement of glossopharyngeal, vagal, trigeminal, and facial nerves—together with the “onion-skin” sensory pattern localizing the lesion to the spinal trigeminal nucleus/tract—suggests a brainstem-level process. The close anatomical proximity of the spinal trigeminal complex to adjacent cranial nerve nuclei and ganglia provides a plausible mechanism for contiguous viral spread and the stepwise neurological progression.This presentation parallels Ramsay Hunt syndrome (RHS), in which VZV reactivation may precede delayed cranial nerve deficits. Similarly, pharyngo-laryngeal zoster may serve as a prodromal sign of delayed, multiple cranial or autonomic neuropathies. As in RHS, early corticosteroid therapy may have contributed to the rapid improvement in both neuropathic and autonomic dysfunction. From a hospital medicine perspective, this case highlights the importance of close and serial neurological examinations in patients with suspected VZV reactivation. Despite an initially localized presentation, this patient developed multiple new neurological deficits after admission, underscoring the need for continued vigilance even after antivirals are initiated.
Conclusions: Pharyngo-laryngeal zoster can progress to multiple cranial and autonomic neuropathies. Hospitalists should maintain a high index of suspicion and perform repeated neurological assessments during hospitalization. Early recognition of evolving deficits and timely corticosteroid therapy may prevent irreversible neurological complications.