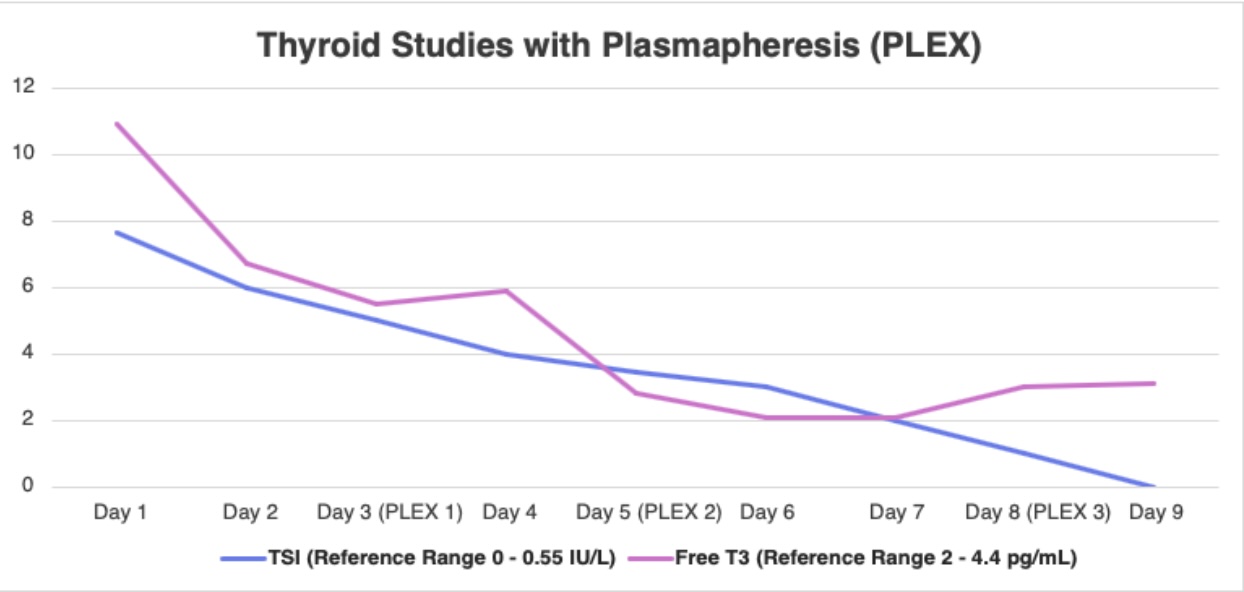
Case Presentation: We report the case of an 80-year-old woman with known Graves disease who presented to a community hospital with atrial fibrillation with rapid ventricular response and congestive symptoms following a respiratory infection. Despite aggressive initial medical therapy which included beta-blockade, high-dose methimazole, corticosteroids, and cholestyramine, the patient demonstrated persistent tachyarrhythmia and clinical instability. Her course was further complicated by hypotension limiting beta-blocker use and development of coagulopathy. Recognizing refractory thyroid storm, the hospitalist team rapidly coordinated multidisciplinary involvement among endocrinology, cardiology, and critical care. Despite maximal pharmacologic therapy, the patient showed minimal improvement and was transferred to the ICU for therapeutic plasmapheresis. Following plasmapheresis, the patient’s thyroid function and hemodynamics significantly improved, allowing de-escalation of methimazole and steroids, stabilization of heart rate, and transfer back to the hospitalist service for ongoing management.
Discussion: Thyroid storm is a rare but life-threatening endocrine emergency requiring rapid recognition and aggressive management. This case highlights the unique challenges of treating refractory thyroid storm in a community hospital, where timely multidisciplinary coordination becomes critical. Despite guideline-directed therapy— including beta-blockade, thionamides, iodine, corticosteroids, and supportive care, our patient remained in atrial fibrillation with rapid ventricular response and developed worsening coagulopathy, indicating severe, treatment-resistant disease. The decision to escalate care to therapeutic plasmapheresis, facilitated through collaboration between hospital medicine, endocrinology, intensive care, cardiology, resulted in marked clinical improvement. This case demonstrates the importance of early recognition of refractory features, the need for a structured, team-based approach, and the feasibility of implementing advanced therapies such as plasmapheresis even within community hospital environments. It further reinforces existing evidence that plasmapheresis can be lifesaving in cases where conventional therapy fails, offering a bridge to stabilization while awaiting metabolic recovery.
Conclusions: This case underscores the essential role of hospitalists in orchestrating early multidisciplinary collaboration in the management of severe thyroid storm, particularly in resource-limited community hospital environments. Prompt recognition of treatment-refractory disease and timely escalation to therapies such as plasmapheresis were critical to the patient’s recovery. This report highlights the value of structured multidisciplinary pathways to improve outcomes in a complex endocrine emergency.