Background: Transthoracic echocardiography (TTE) is a clinical tool for cardiac evaluation of hospitalized patients but is frequently associated with a greater hospital length of stay.1 At our institution, delays in TTE completion have been attributed to a shortage of sonographers and overutilization by inpatient teams for certain clinical conditions. From January to October 2023, only 40% of inpatient TTEs on the medicine service were completed within 24 hours. We propose that point-of-care ultrasonography (POCUS) can triage inpatient TTE necessity using limited, qualitative assessments. Studies have demonstrated that trained hospitalists and internal medicine residents can safely perform and interpret cardiac POCUS exams with non-inferiority to cardiologists for specific clinical indications.2–4
Purpose: To demonstrate the feasibility of a POCUS-guided TTE triage protocol that increases the proportion of TTEs completed within 24 hours.
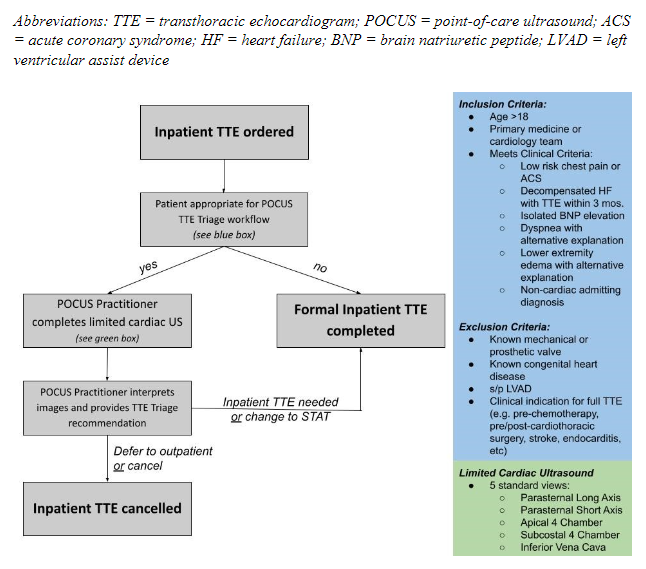
Description: First, we conducted an institutional clinician needs assessment about TTE delays and its impact on clinical work using standard Likert Scale responses. A triage protocol and patient selection criteria were developed by consensus between hospitalist and cardiology representatives (Figure 1). POCUS practitioners included hospitalists and internal medicine residents who had completed or were in the process of a society-sponsored POCUS certification pathway. POCUS practitioners identified and scanned appropriate patients using a convenience sample approach; deidentified images were stored on a cloud-based databank. Then, they completed a questionnaire including a brief clinical history, TTE indication, interpretation of key findings, and TTE triage recommendation. Two cardiologists reviewed the POCUS images and clinical history, then completed their own image interpretation and TTE triage recommendation for comparison.
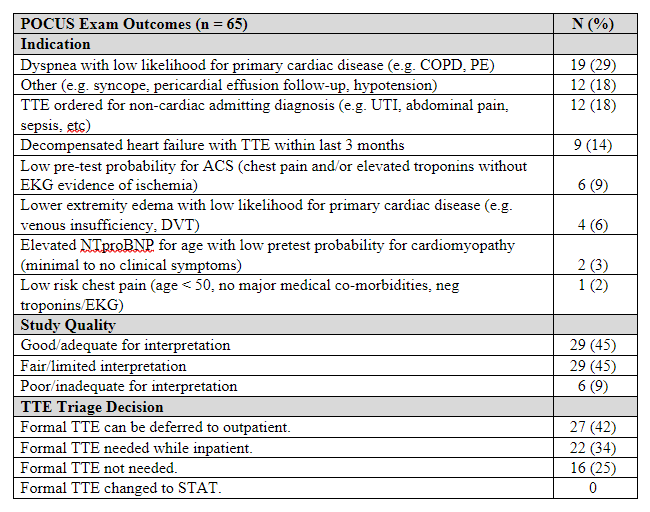
Conclusions: The needs assessment was completed by 153 respondents: 49 (32%) internal medicine residents, 61 (40%) hospitalists, 32 (21%) cardiologists, and 11 (7%) attendings from other divisions. Overall, clinicians perceived that diagnostic testing was not performed in a timely manner, particularly amongst cardiologists compared to other groups. Additionally, respondents were receptive to POCUS use in triaging TTE orders, though favored following certified users’ recommendations to using it themselves. POCUS practitioners completed 65 studies over 10 weeks (Table 1); 58 (90%) studies were deemed satisfactory for at least limited interpretation. Forty-three (67%) studies identified through the triage protocol were recommended to be deferred to outpatient or canceled altogether. The two most common TTE indications for POCUS triage were dyspnea and requests in patients with non-cardiac primary admitting diagnoses. We conclude that a POCUS-guided TTE triage protocol is feasible to reduce inappropriate inpatient TTE orders for certain clinical conditions, which is likely to reduce delays in inpatient TTE completion.