Case Presentation: A 46-year-old woman presented with left hemiparesis following elective hip replacement. Past medical history noted essential hypertension currently untreated and bilateral hip dysplasia corrected as a child. She took ibuprofen and hydrocodone-acetaminophen for pain. She was adopted at age two. She smoked a half pack of cigarettes daily.
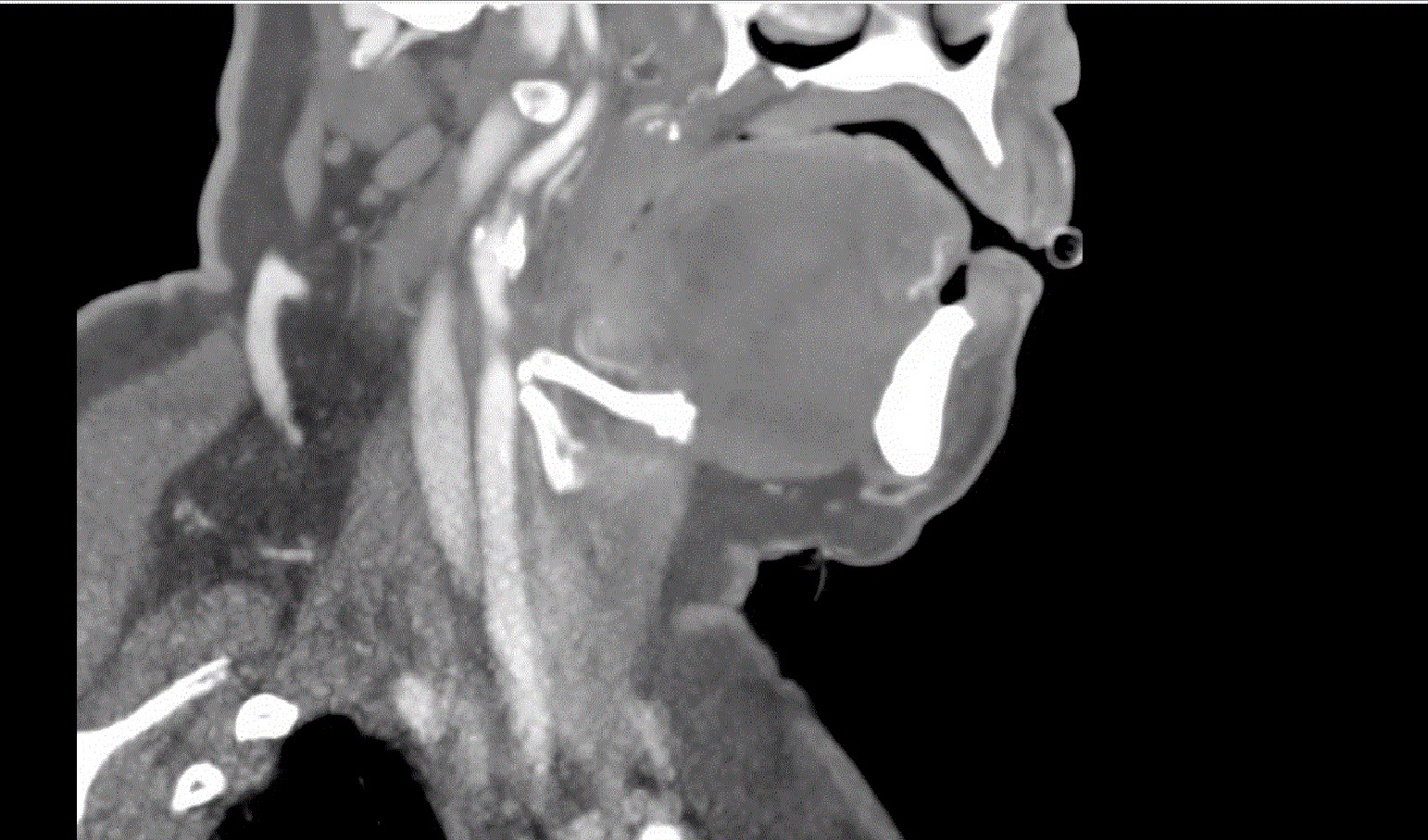
Right total hip arthroplasty was completed successfully. Post operatively she developed left sided weakness. She was hypotensive and received IV fluids. Blood pressure was unable to be obtained in the right arm but left arm BP was 161/91mmHg. CTA of the head and neck showed critical stenosis of the right internal carotid artery; her right subclavian artery was also stenosed. She received aspirin 325mg. Permissive hypertension was initiated. MRI of the brain noted diffusion restriction throughout the right cerebral hemisphere suggestive of a watershed infarct. She underwent carotid endartectomy on post-operative day four.
Hospital medicine was consulted for management of hypertension. She was 1.53m tall, weight 68.5kg, BMI 29kg/m2, with broad shoulders. She had an ejection systolic murmur 3/6 loudest in right upper sternal border with radiation to the carotids; right radial pulse was reduced. She had a left hemiparesis. Gynecological history revealed irregular menses and no pregnancies. Echocardiogram revealed a bicuspid aortic valve with mild stenosis, mild aortic root dilation.
Anti-hypertensive management was initiated, as well as aspirin and atorvastatin. She was counseled on smoking cessation and discharged to inpatient rehabilitation. Given her history and her physical findings Turner syndrome was considered and karyotyping revealed mosaicism with 45,X, 47,XXX, 46,XX.
Discussion: Hypertension and cerebrovascular disease are common conditions seen in Hospital Medicine. Turner Syndrome is one of the most common chromosomal abnormalities, seen in around 1 in 2500 female births. About half have monosomy X and the other half have partial absence, translocation of the X chromosome, or mosaicism. 1 It is usually diagnosed in childhood or adolescence due to delayed growth, failed puberty or infertility.
This case represents an extremely late presentation of Turner Syndrome. This was likely a result of her adoption, subsequent estrangement from her family and intermittent medical care. Her choice not to pursue pregnancy may have contributed. Up to 10% of patients with Turner syndrome have spontaneous menstruation and 5% childbirth.2 A mosaic pattern of gene expression may alter phenotypical presentation and prevent earlier recognition. Congenital heart disease is found is about half of patients with Tuner syndrome.3 Accelerated vascular disease is likely due to a combination of estrogen deficiency, metabolic syndrome and genetic factors.4
Conclusions: Genetic causes should be considered in the presentation of early cardiac disease and hypertension. Early recognition may prevent morbidity and mortality by early intervention for vascular abnormalities.