Background: Migraine headache is a common pediatric disorder frequently leading to hospital admission. Inpatient migraine headache treatment involves increasingly complex treatments, including fluid resuscitation and a variety of medications and therapies. Our previous study(1) has shown that the cost of inpatient treatment for pediatric migraine headache is increasing at a higher rate than reported overall healthcare costs over the past decade. The objective of this study was to identify specific departmental areas of increasing cost with potential for cost-savings for patients hospitalized with migraine headache at pediatric hospitals across the United States.
Methods: We performed a retrospective cohort study of patients ages 1-18 years, with ICD 9 and 10 codes for migraine headache as the principal diagnosis, admitted to tertiary care childrens’ hospitals in the USA between 2010 and 2018. Hospital-level case-average length of stay (LOS) and case-average departmental charges were extracted from the Pediatric Health Information System (PHIS) database Key Performance Indicator reports. Trends in ALOS and charges were examined using linear regression analyses. The study was approved by the IRB.
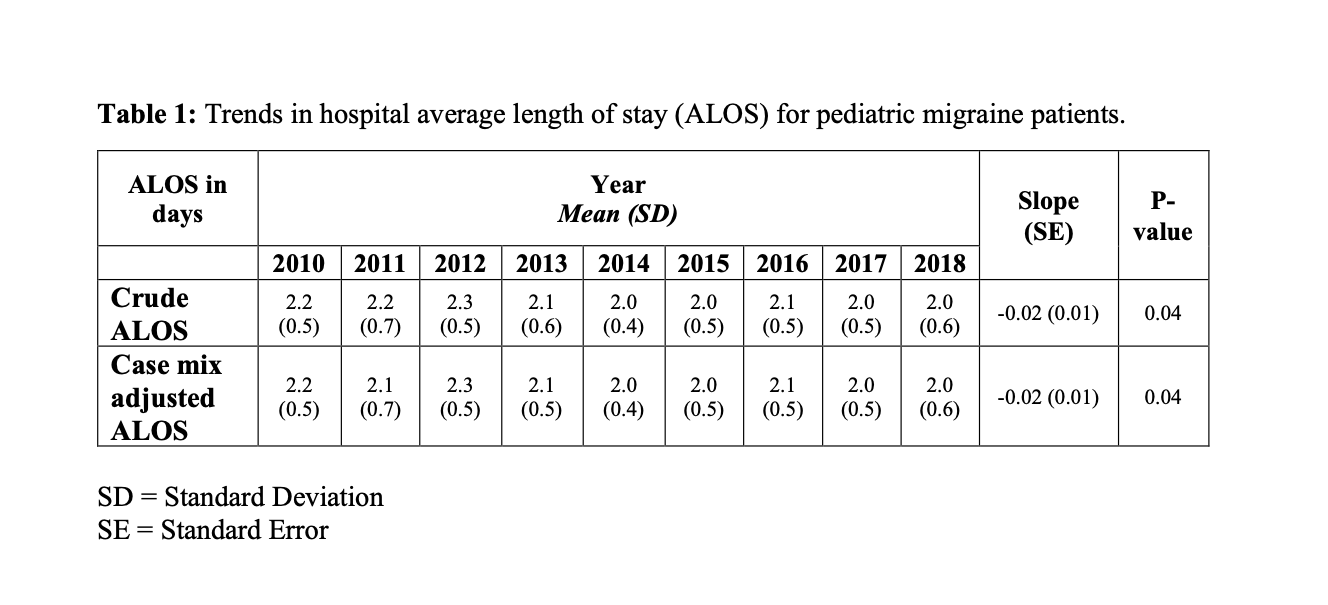
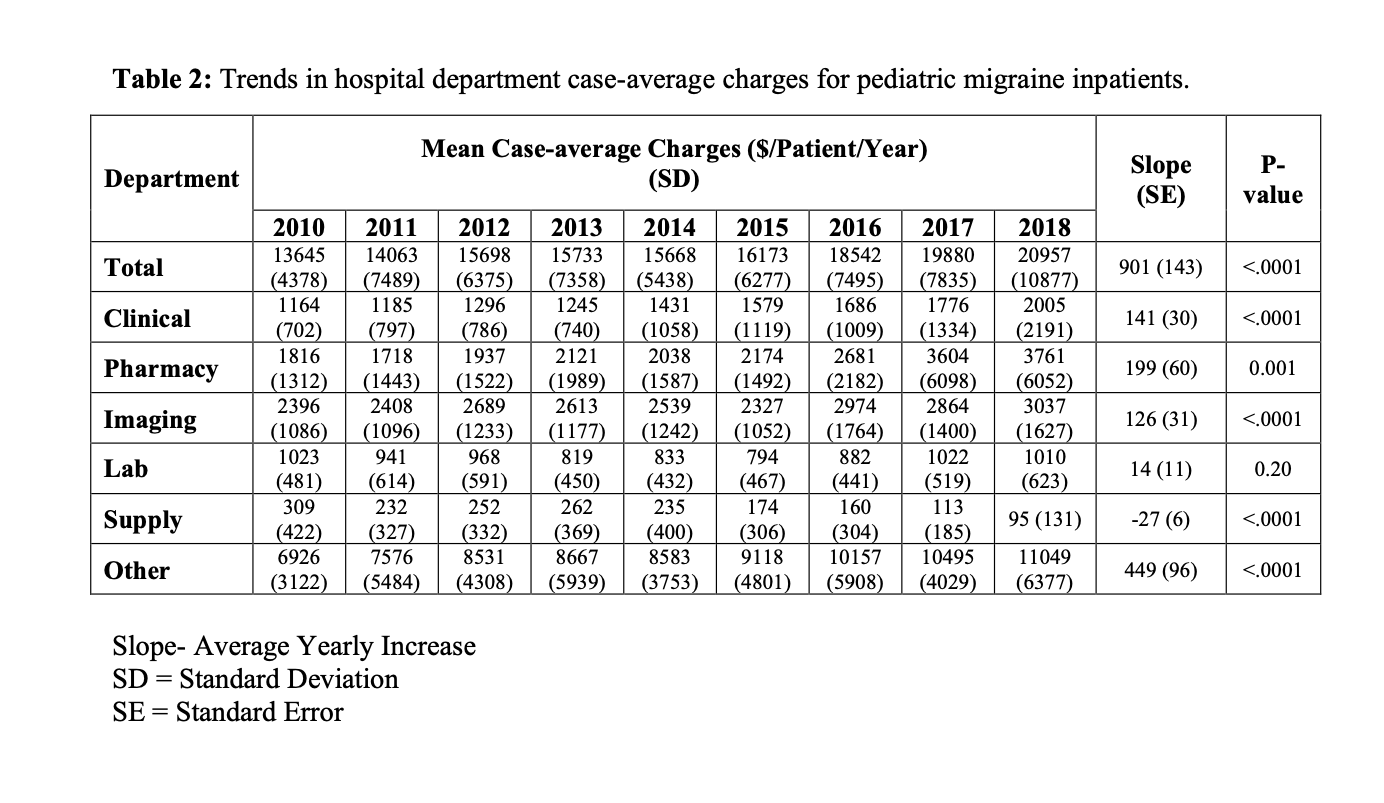
Results: A total of 38 hospitals each provided yearly data, for a total of 18,772 eligible patients during the study period. The mean (standard deviation) average LOS decreased significantly from 2.2 (± 0.5) to 2.0 (±0.6) days between 2010 and 2018, with significance retained after case-mix adjustment (Table 1). In contrast, overall charges significantly increased by an average of $901 (±$143) per patient per year during the study period (Table 2). The largest yearly departmental cost increase was $449 (± $96) for charges classified as “Other” (room, board, and emergency department (ED) charges). Significant cost increases were also noted for clinical services, pharmacy, and imaging, while supply costs decreased (Table 2).
Conclusions: While average length of stay has decreased, the cost associated with inpatient treatment of migraine headache has increased. A steady increase in imaging and pharmacy charges is apparent, however our data does not clarify whether this reflects an increase in use or in unit cost. Further study is needed to determine if use has increased, thereby providing an avenue for cost-saving efforts. More than half of the cost increase was driven by the daily cost of room, board and ED visits. While inpatient clinicians cannot directly influence these hospital charges, streamlining care to further decrease average LOS and avoid admission via the ED may indirectly provide meaningful cost savings for children hospitalized for treatment of migraine headaches.