Background: Many patients with chronic obstructive pulmonary disease (COPD) have suboptimal peak inspiratory flow rate (sPIFR) because of lung hyperinflation, hypoxemia, and muscle wasting, preventing effective use of dry powder inhalers commonly used to treat COPD. sPIFR and airflow limitation interaction may be responsible for excess symptoms in patients with COPD. Here we characterize baseline demographics and clinical characteristics of patients with COPD according to their PIFR (suboptimal, borderline [bPIFR] or optimal [oPIFR]) to DISKUS® resistance (PIFRD) and Global Initiative for Chronic Obstructive Lung Disease (GOLD) airflow categories (forced expiratory volume in 1 second [FEV1]; 50–79% predicted [GOLD 2], 30–49% predicted [GOLD 3], and <30% predicted [GOLD 4]).
Methods: Baseline characteristics, PIFRD, FEV1, and forced vital capacity (FVC) data from 2 randomized controlled phase 3 trials (NCT03095456; NCT02518139) were pooled to compare population differences between PIFR subgroups and airflow categories.
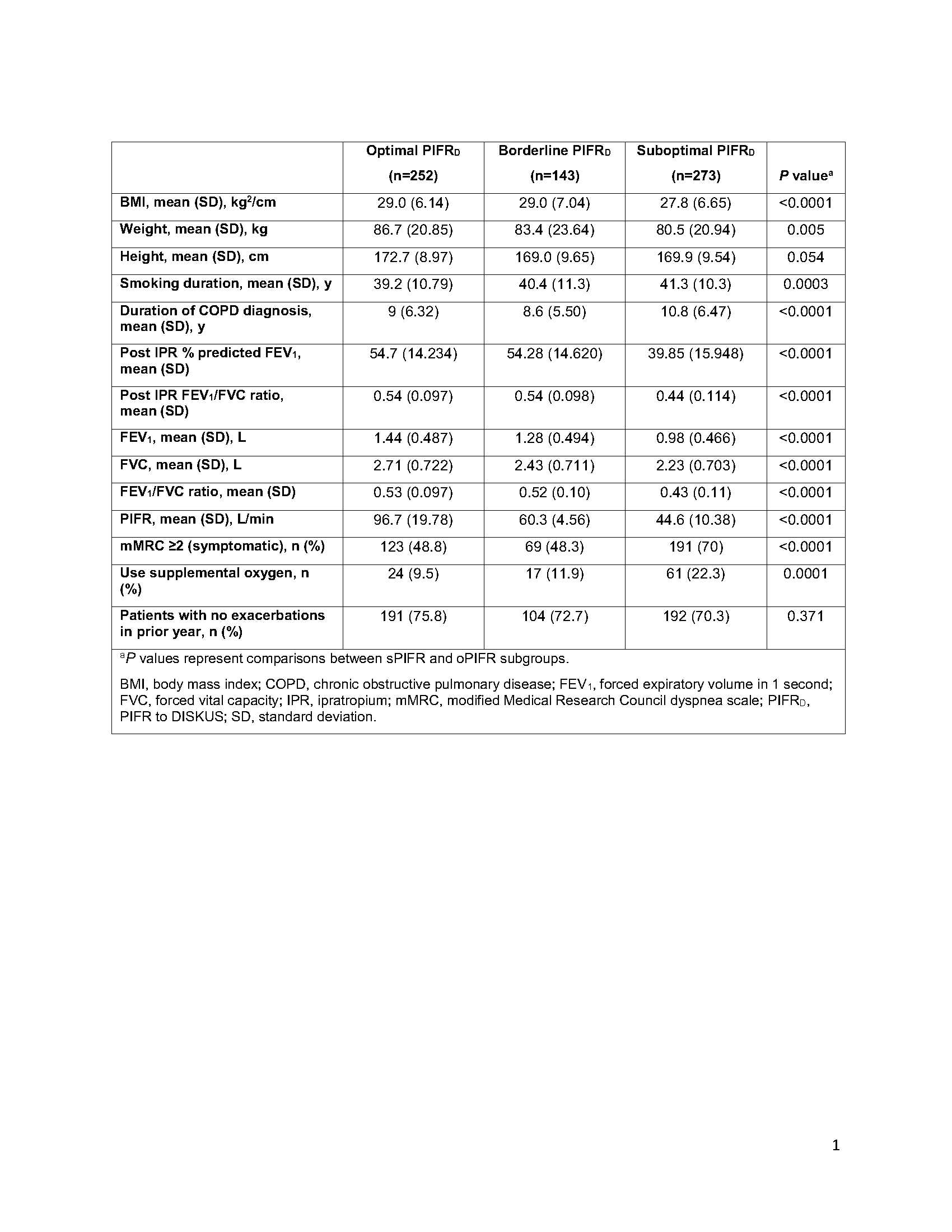
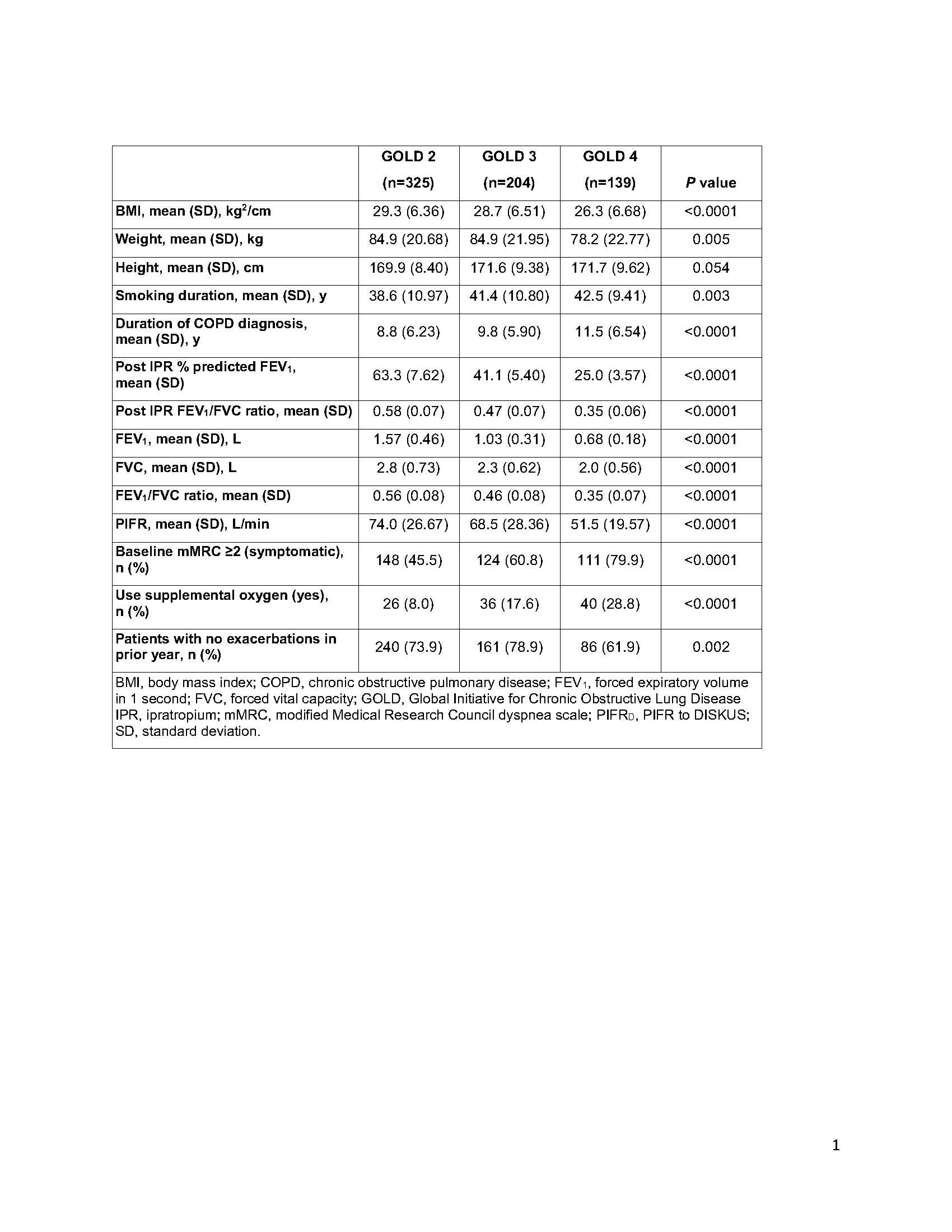
Results: Of 668 patients with evaluable PIFRD measurements, 273 (41%) had sPIFRD, 143 (21%) had bPIFRD, and 252 (38%) had oPIFRD. Most patients were white (93%) and male (60%) with a mean (range) age of 65 (41–87) years; 45% of patients were current smokers and 56% were taking inhaled corticosteroid/long-acting beta agonist combination treatment. Patients with sPIFR had smaller stature (lower height, weight, and body mass index [BMI]) and longer smoking history and duration of COPD compared with patients with oPIFR (Table 1). sPIFR was also associated with lower lung function (FEV1, FVC, FEV1/FVC), higher use of supplemental oxygen, and more symptomatic disease (Table 1). Patients with bPIFR generally had characteristics similar to both patients with sPIFR and oPIFR. sPIFR was present in all airflow categories with prevalence increasing from 24% of patients in GOLD 2 to 81% in GOLD 4. Weight, BMI, lung function, and PIFR were lower for patients with higher airflow limitation, whereas use of supplemental oxygen and symptom load were higher (Table 2).
Conclusions: These clinical trial data showed presence of sPIFR in patients with moderate to very severe COPD. Patients with sPIFR had more severe airflow obstruction at baseline than patients with bPIFR or oPIFR. Prevalence of sPIFR increased with disease severity. Thus it may be beneficial to measure both PIFR and airflow limitation before considering treatment options for patients with COPD.