Background: Healthcare has a significant environmental footprint, accounting for approximately 8.5% of U.S. carbon emissions1. Metered dose inhalers (MDIs) contribute to this footprint through hydrofluoroalkane propellants, which are potent greenhouse gases (GHGs). Compounding this issue, MDIs leak GHGs even when not in use, making their total volume, both used and unused, a factor in healthcare’s carbon footprint2. Inhalers are common practice at our hospital, both for rescue and as a continuation of home medications. Our aim is to reduce inefficiencies in inpatient MDI management by reducing unnecessary as needed (PRN) orders and preventing device loss during patient transfers.
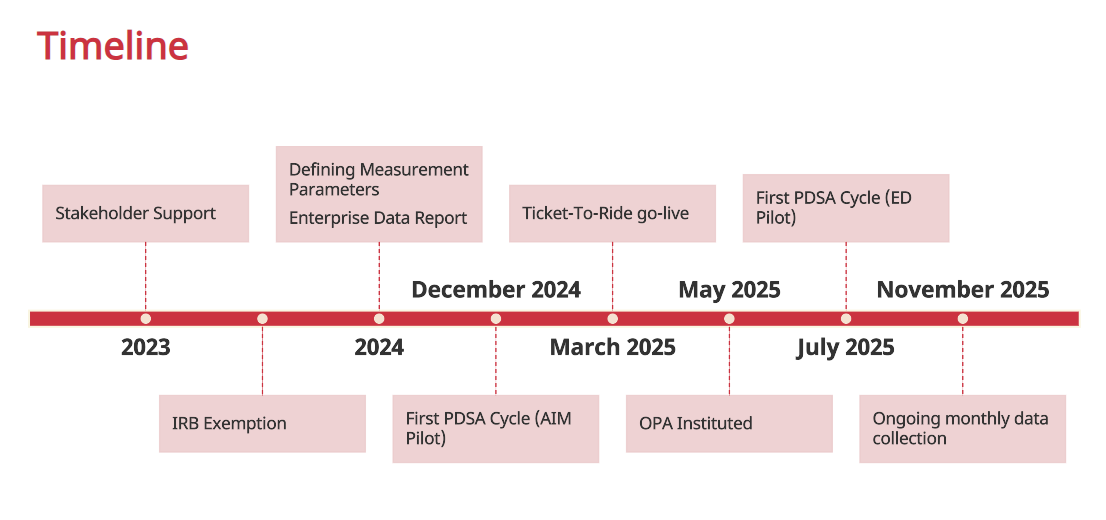
Methods: This quality improvement (QI) project at MaineHealth Maine Medical Center (MMC) included two groups of interventions: one targeting adult inpatient medicine providers and one system-wide change. From Dec 202 to Jan 2025, we launched an educational campaign (lectures, signage) targeting adult Hospital Medicine teams, including residents. In April 2025, we introduced an Our Practice Advisory (OPA) in the electronic medical record, which aimed to discourage the unnecessary continuation of home PRN albuterol inhalers during admission medication reconciliation. In March 2025, we updated the existing institutional Ticket-to-Ride form to include multidose medications. This change addressed transfer-associated device loss and was paired with a four-week education campaign in the emergency department. We used premature re-dispensation—defined as issuing an inhaler before its expected refill date—as a proxy for device loss. Data came from the electronic health record via enterprise reporting tools, and carbon impact was calculated using published methods3. The MaineHealth IRB deemed this project “not research.”
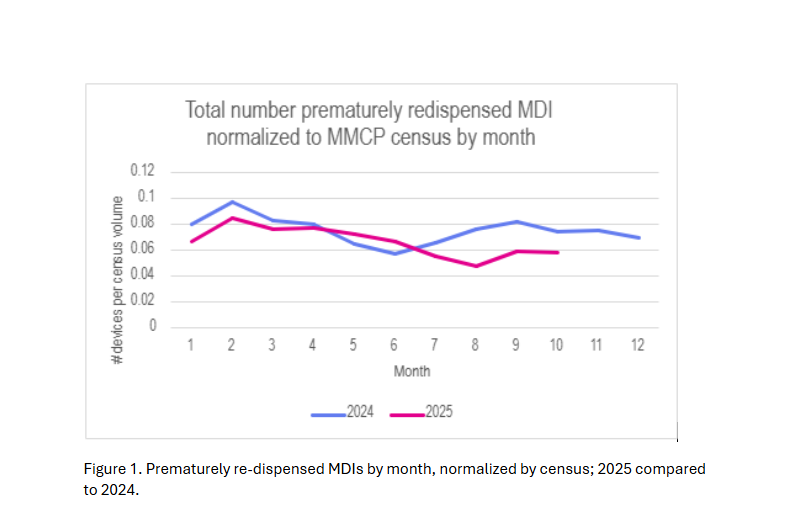
Results: In FY24, a total of 2,779 MDIs were prematurely re-dispensed on inpatient units. For the most frequently impacted inhalers, this represents a total annual carbon footprint of 27,934 kg CO2e, equivalent to 3,143 gallons of gasoline, and an associated cost of $68,805. Forty-five percent of premature re-dispensation occurred around the time of transportation between units. Following implementation of the OPA and changes to the Ticket-to-Ride, with accompanying education campaign, the total number of prematurely re-dispensed devices decreased and has been sustained (figure 1). Comparing 2024 to 2025 totals to date for the top three inhaler types we found environmental savings of 2565 kg CO2e, which is equivalent to 289 gallons of gasoline, and financial savings of $6,912.
Conclusions: This QI project in process highlights the contribution of prematurely re-dispensed inpatient MDIs to financial and environmental waste. Addressing this issue can reduce emissions and costs without compromising care. We intend to continue measuring data through the end of December 2025 to assess whether the changes are sustained and collect culture change surveys from the Hospital Medicine providers and pharmacy technicians.