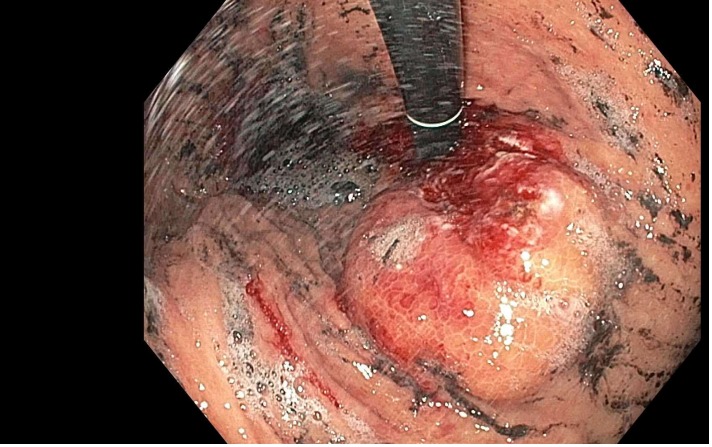
Case Presentation: 61-year-old male presented with fatigue, dizziness and epigastric discomfort. Patient was noted to be anemic on lab investigations. Patient underwent a CT scan of the abdomen and pelvis which demonstrated a 4.7 x 4.6 cm mass in the anteromedial stomach distal to GE junction. There was also a 1.8 x 1.5 cm structure medial to the mass, likely a gastrohepatic lymph node. Patient underwent endoscopy which demonstrated a submucosal mass in the cardia with associated ulceration and active bleeding. Hemostatic clips, bipolar cautery, and hemostatic spray were done to maintain hemostasis. Repeat EGD with endoscopic ultrasound/biopsy demonstrated the known large infiltrative and submucosal mass. The lesion was noted to be below the gastroesophageal junction with no evidence of esophageal masses. It was noted that the lesion which was in the cardia of the stomach appeared to be within the wall and measured 4.6 cm in maximal thickness. There was an adjacent malignant appearing lymph node in the perigastric region measuring 2 x 1.2 cm. FNA biopsy pathology report demonstrated squamous cell carcinoma. Patient underwent neoadjuvant chemoradiation. Patient underwent concurrent chemotherapy with carboplatin/paclitaxel. His chemotherapy treatment was later switched to concurrent capecitabine (due to developement of cardiac arrest when receiving paclitaxel) for the duration of his radiation. Radiation treatment was completed. PET scan did not reveal any distant metastasis. Patient is currently scheduled for surgery consisting of partial gastrectomy, omentectomy, lymph node dissection, and dual reconstruction.
Discussion: Squamous cell carcinoma of the stomach is an extremely rare entity. Prior literature is limited to case reports/case series. Currently the pathogenesis of this malignancy is very poorly understood, multiple theories have been postulated including viral infection/chronic inflammation as a precipitant. Treatment mostly revolves around chemotherapy/radiotherapy/surgical resection. Prognosis is poor as compared to other primary carcinomas of the stomach such as adenocarcinoma. In our case we have attempted all 3 modalities. In our case PET scan did not show any evidence of distant metastasis which gives opportunity for surgical resection. Due to the extent of the disease (lymph node positive) and active bleeding, it was determined that chemotherapy and radiation would be the best option however the patient could not continue with carboplatin and paclitaxel as he developed cardiac arrest while receiving paclitaxel in an outpatient infusion center. Capecitabine was felt to be the safest and least myelosuppressive, yet best radiosensitizer for this patient. Yet, despite completion of chemo/XRT, imaging showed persistent disease and patient’s symptomatic anemia had returned. Given the rarity of this condition there is no set treatment algorithm. Our approach employed all the above prior treatments from previous literature.
Conclusions: Squamous cell carcinoma of the stomach is a very poorly understood malignancy. The rarity of his presentation along with scarce literature make it challenging disease to treat.