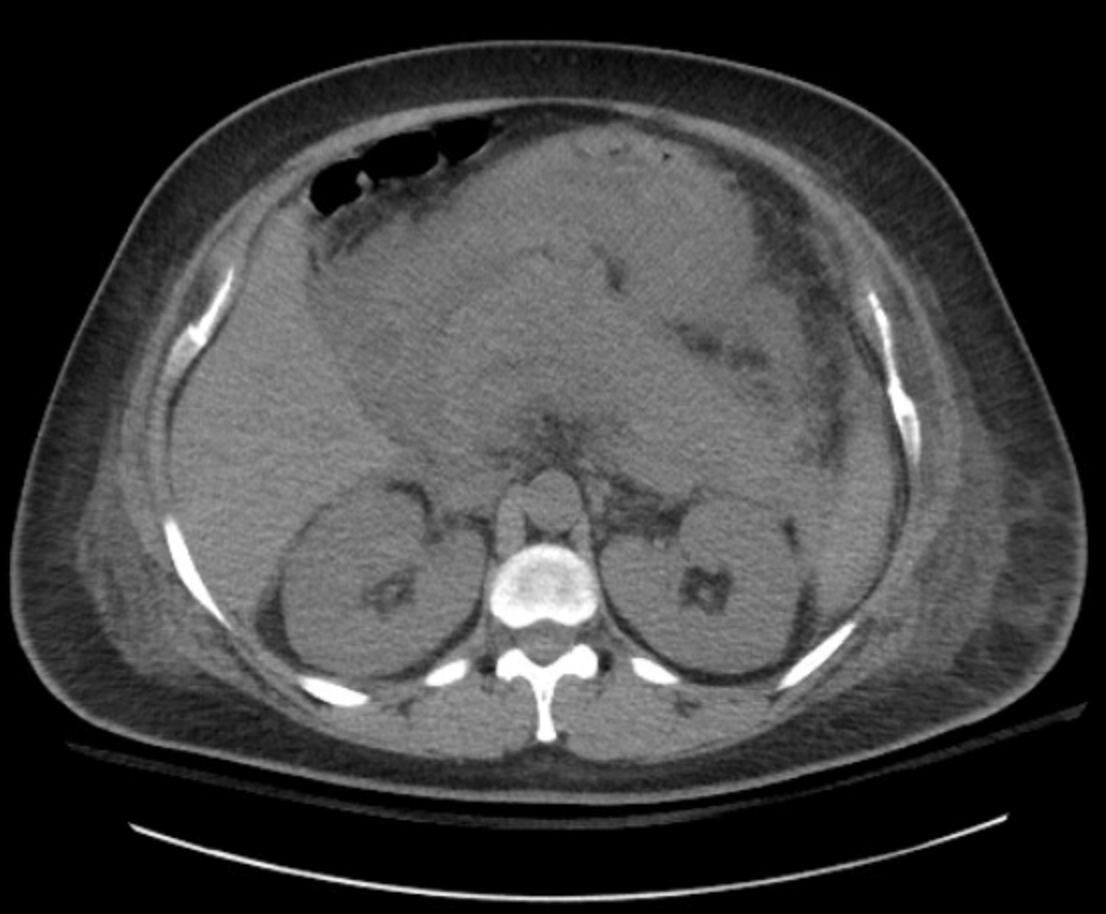
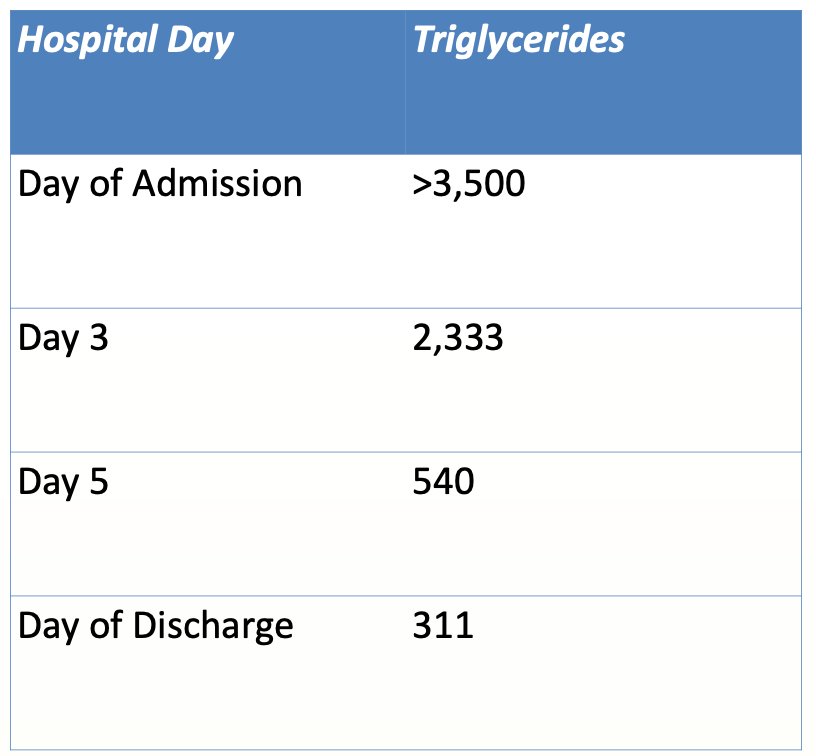
Case Presentation: A 38-year-old female with a past medical history of recurrent pancreatitis, heart failure with recovered ejection fraction, type 2 diabetes mellitus, and hyperlipidemia presented with acute-onset abdominal pain, nausea, and vomiting. Her history was notable for no alcohol use, a prior cholecystectomy, and an episode of pancreatitis with an unclear cause several months prior. Physical exam demonstrated a patient in mild distress with epigastric tenderness and guarding. Labs showed a lipase greater than 6,000 U/L and CT scan of the abdomen demonstrated edema in the head and neck of the pancreas consistent with pancreatitis. Additional workup was notable for a triglyceride level of greater than 3,500 mg/dL and a low ionized calcium of 2.9 mg/dl. The patient initially received intravenous insulin at an outside hospital. At our hospital, she was started on intravenous fluids, pain control, and admitted to the ICU for further management and insulin therapy. Her ICU course was complicated by acute kidney injury requiring temporary hemodialysis. She received plasmapheresis with eventual reduction in her triglyceride levels and resolution of her pancreatitis. She was discharged on gemfibrozil.
Discussion: The risk for hypertriglyceridemia-induced pancreatitis (HTGP) increases significantly with triglyceride levels over 1000 mg/dL. The pathophysiology is believed to involve pancreatic lipase, which is released from acinar cells in the vascular bed of the pancreas. This enzyme cleaves triglycerides (TG) into free fatty acids, which induce a toxic effect on the acinar cells and capillary endothelium, thereby precipitating an inflammatory cascade within the pancreas. Furthermore, high levels of chylomicrons seen in hypertriglyceridemia increase viscosity in the pancreatic vasculature, leading to capillary plugging, ischemia, and potentially acidosis. Initial treatment for HTGP is similar to management of acute pancreatitis due to other causes and includes bowel rest, intravenous hydration, and pain control. Intravenous insulin therapy lowers triglyceride levels by activating lipoprotein lipase. Another approach is to use plasmapheresis in hospitalized patients, which is estimated to reduce the serum TG level by 49%–80%. However, current literature supporting the use of plasmapheresis in HTGP in the hospital is from observational studies with a lack of randomized controlled trials. Additionally, this treatment has higher costs and need for staffing, which can limit the use of this approach depending on the hospital system. Furthermore, the benefit of early initiation of plasmapheresis is still in question.
Conclusions: We present this case to highlight the need to consider hypertriglyceridemia as a potential cause for pancreatitis and subsequent multi-organ failure. Our case also demonstrates a multimodal approach to help lower serum triglyceride levels in severe HGTP, but more data is needed regarding the combined use of insulin and plasmapheresis in terms of prognosis and mortality. Furthermore, further research is needed to validate the benefits of early initiation of plasmapheresis.