Background: Hospital medicine physicians (hospitalists) are essential to inpatient care delivery and coordination. As the population grows and ages, demand for hospital-based care continues to rise, raising concerns about whether the current workforce can meet future needs. Despite the central role of hospitalists in quality, efficiency, and patient safety, few studies have projected long-term workforce adequacy or identified where shortages may be most severe.
Methods: We conducted a national workforce forecasting analysis using the Health Workforce Simulation Model (HWSM) developed by HRSA’s National Center for Health Workforce Analysis. The model estimates annual supply and demand for full-time equivalent (FTE) hospital medicine physicians at the national, state, and metropolitan versus nonmetropolitan levels, with metro/nonmetro categories defined using HRSA’s standard county-based rurality classification. Projections spanned 2022–2037 under two demand scenarios: (1) status quo (current utilization patterns) and (2) reduced barriers (improved access for underserved populations). Supply forecasts incorporated training inflows, attrition, and retirement patterns. Descriptive statistics and visualization were used to evaluate supply, demand, and adequacy (supply-to-demand ratio) across geographic settings.
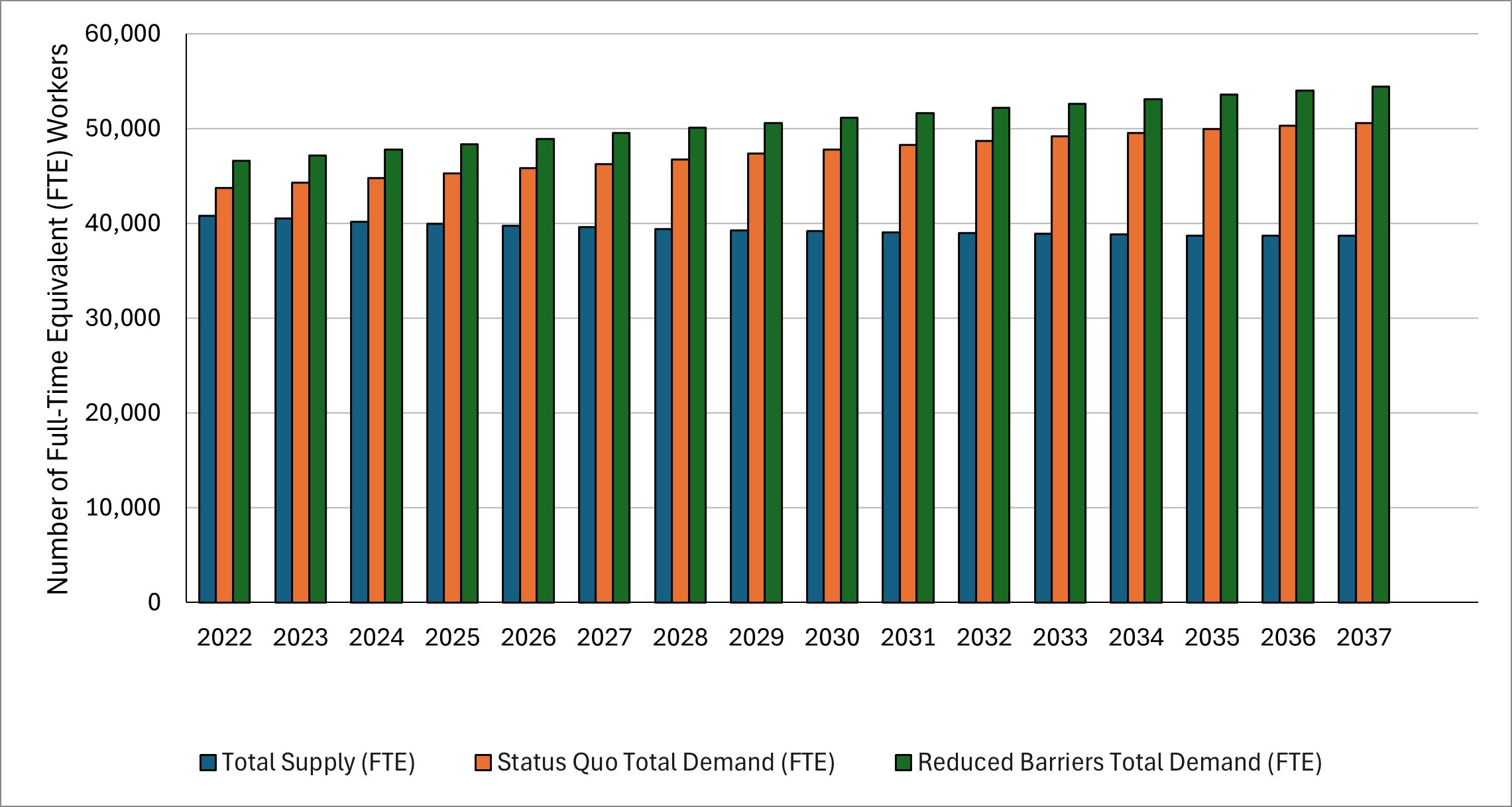
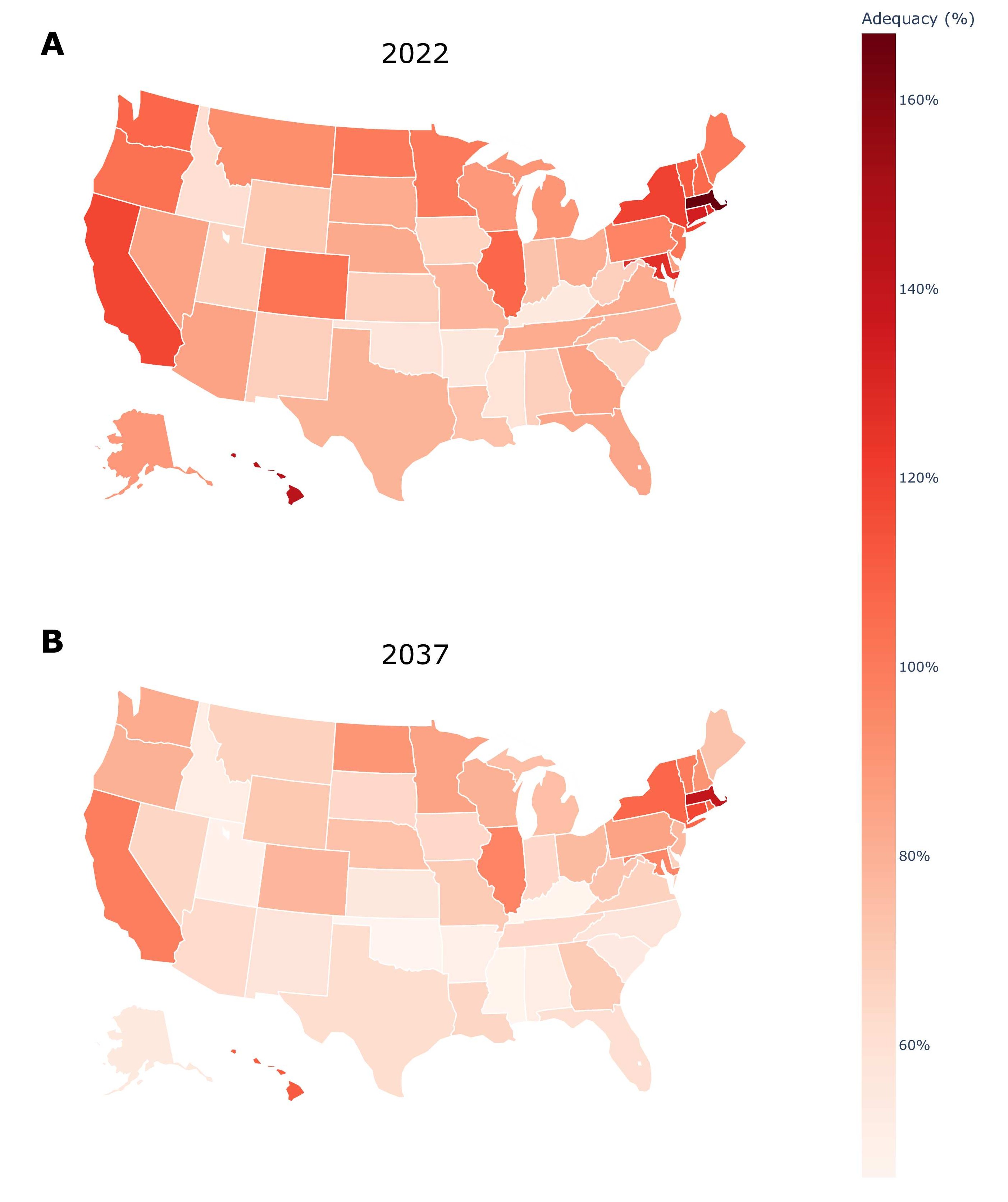
Results: In 2022, the U.S. hospital medicine workforce included 40,810 FTEs, with demand of 43,730 under the status quo and 46,640 under reduced barriers. By 2037, supply is projected to fall to 38,700 (–5.2%) while demand rises to 50,600 (+15.7%) under the status quo and 54,410 (+16.7%) under reduced barriers, expanding the national shortfall to 11,900–15,710 FTEs (Figure 1). National adequacy correspondingly declines from 93% to 76% under the status quo and from 88% to 71% under reduced barriers. Compared with 37 HRSA-modeled specialties, hospital medicine ranks among the lowest, falling to 30th in projected workforce adequacy by 2037. Metro and nonmetro trends diverge substantially: metro supply decreases modestly from 37,860 to 36,070 FTEs (–4.7%), while nonmetro supply declines nearly twice as rapidly, from 2,950 to 2,630 FTEs (–10.8%). Adequacy mirrors these patterns, with metro adequacy falling from 103% to 83% and nonmetro adequacy dropping from 55% to 36%. State-level variation is substantial—15 states had workforce surpluses (>100% adequacy) in 2022, but only six are projected to remain above adequacy by 2037 (Figure 2). The District of Columbia maintains the highest adequacy (256% in 2037), whereas Kentucky and Mississippi fall to the lowest levels (47%).
Conclusions: Substantial and widening hospitalist shortages are projected through 2037, threatening inpatient capacity and care access, particularly in rural and underserved regions. These findings underscore the urgency of proactive workforce planning and policy intervention. Expanding graduate medical education positions, supporting retention and wellness initiatives, and optimizing team-based models with advanced practice providers may help offset projected deficits. Sustained investment in workforce planning is essential to maintain the value, safety, and equity of hospital care nationwide.