Background: Introduction: Colorectal cancer is the 4th most common cancer in the United States. It is the second most common cause of death in the united states. Despite universal advocacy for screening colonoscopies and early diagnosis, disparities in screening and diagnosis of colorectal cancer exist which affects outcomes. In this analysis, we determine racial disparities and treatment outcomes for colorectal cancer treatment in the united states.
Methods: Methods: We performed a retrospective analysis of the National Inpatient Sample database (NIS). Patients with a primary diagnosis of colorectal cancer who were 18 years and older were included. Multivariable analysis was used to determine the effect of race on receiving a therapeutic procedure (either open surgical procedure, or laparoscopy/robotic procedure) and hospitalization outcomes as it relates to patient’s mortality. We adjusted for patients age, sex, number of comorbidities (elixhauser comorbidity score), insurance type and hospital level characteristics (i.e.States size, teaching status) and location (urban or rural location).
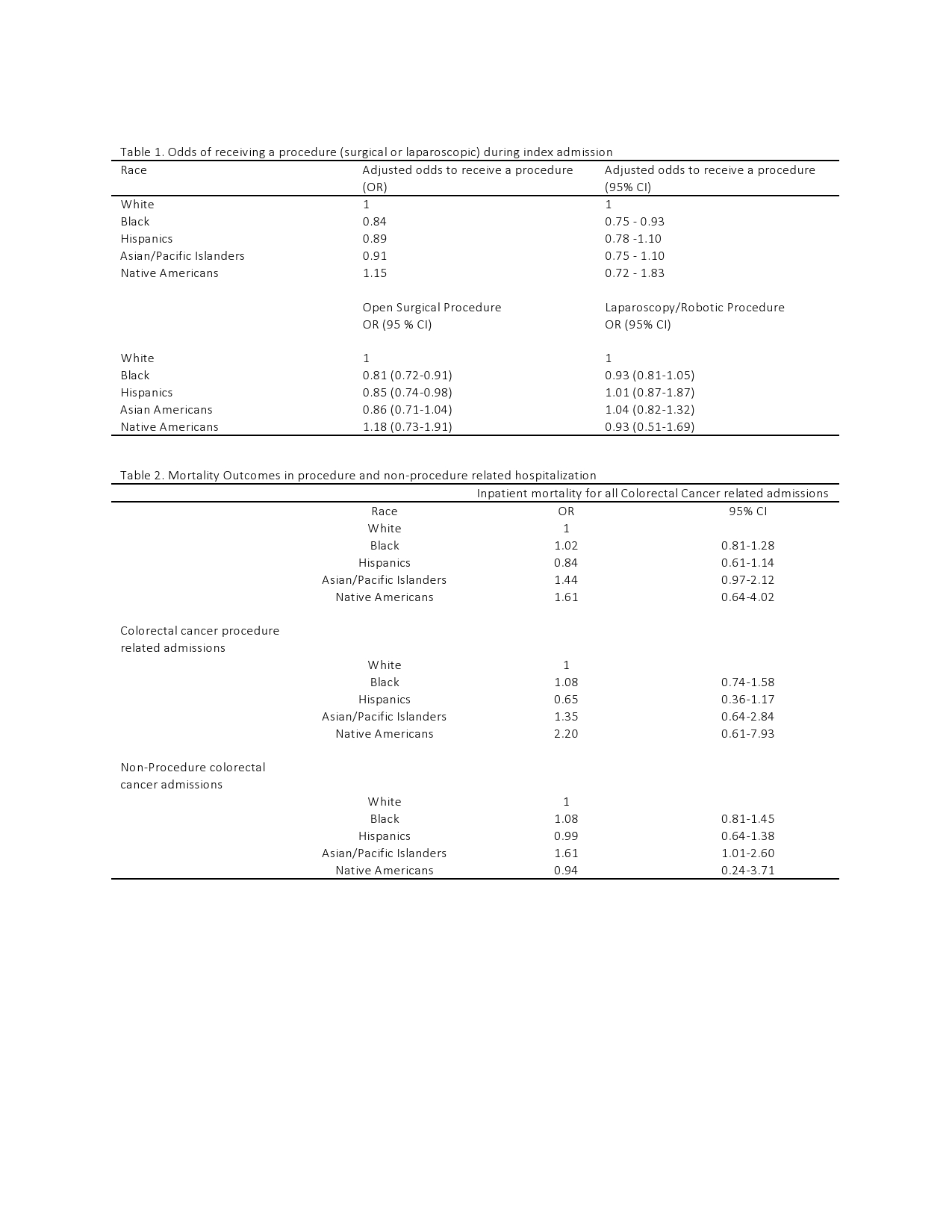
Results: Results: There were 25,749 discharge diagnosis of colorectal cancer in the United States in 2014 of which 19,300 were associated with undergoing a procedure for colorectal cancer treatment. Whites accounted for the majority of colorectal cancer admissions (65%) while blacks 11.4 %, Hispanics 8.0%, Asian/Pacific Islanders 3.2 % and Native Americans 0.4%. Blacks had the lowest frequency of procedure-related admissions and were less likely to undergo a therapeutic procedure relating to colorectal cancer treatment (67.5 vs 76.6 OR 0.84 CI 0.75 – 0.93) compared to whites. For specific procedures, blacks (OR 0.81, CI 0.72-0.91) and Hispanics (OR 0.85, CI 0.74-0.98) had a significantly lesser odds of undergoing open surgical procedures when compared to whites but were similarly likely (Blacks OR 0.93, CI 0.81-1.05, Hispanics OR 0.84, CI 0.61-1.14) to undergo laparoscopic/robotic surgical procedure. On multivariable analysis, Asian/Pacific Islanders had a significantly higher mortality (OR 1.61 CI 1.01-2.60) for non-procedure related colorectal cancer admissions. However, this increased mortality was not seen in procedure-related colorectal cancer admissions. Overall, after adjusting for potential confounders and treatment, there was no significant variation amongst different races for colorectal cancer mortality in patients admitted to the hospital.
Conclusions: Conclusion: Among patients with colorectal cancer there were no procedure-related mortality differences between various races. However, for some reason, Asian/Pacific Islanders had a significantly higher mortality for non-procedure related colorectal cancer admissions. Further studies are warranted to understand the above findings.