
Case Presentation:
A 50‐year‐old renal transplant patient presented to the emergency room with mild respiratory symptoms. Medications included sirolimus, cyclosporine, and prednisone. Vital signs were temperature 37.9°C, pulse 98/minute, blood pressure 109/64 mm Hg, respiratory rate 24/minute, and O2 saturation 88% on room air. Lung exam revealed diffuse bilateral crackles and wheezing. Blood work revealed severe anemia. A chest x‐ray showed bilateral nodular opacities. A chest CT revealed bilateral multifocal, irregular, nodular opacities. Despite the administration of broad‐spectrum antimicrobials for suspected pneumonia, rapidly progressive respiratory failure ensued. The differential included vasculitis and drug‐induced lung toxicity. Bronchoscopy with bronchoalveolar lavage (BAL) and transbronchial biopsy was performed. Negative BAL fluid cultures ruled out opportunistic infections. Transbronchial biopsy results were consistent with alveolar hemorrhage. Sirolimus and antibiotics were discontinued and high‐dose steroids initiated. The following day she was extubated. Two days later she no longer required supplemental oxygen. After 11 days, a follow‐up chest CT showed complete resolution of the airspace opacities.
Discussion:
Sirolimus, a proliferation signal inhibitor (PSI), arrests the cell cycle in the gap 1–synthesis (G1‐S) phase in T lymphocytes, fibroblasts, endothelial cells, and other cell types. It also prevents activation, migration, and proliferation of vascular smooth muscle cells. The most common side effects are thrombocytopenia, leukopenia, and hyperlipidemia. Several reports of life‐threatening biopsyproven pulmonary toxicity exist. Bronchoalveolar fluid analysis and lung biopsy may reveal several distinct histologic patterns, including lymphocytic alveolitis, lymphocytic interstitial pneumonitis, cryptogenic organizing pneumonia, and focal fibrosis. The pathogenic mechanism of PSI‐associated pulmonary toxicity is poorly understood. The clinical presentation of sirolimus‐associated pulmonary toxicity overlaps with a variety of more common infectious and noninfectious disorders. Its diagnosis remains a challenge, particularly if the patient does not rapidly improve on antibiotic therapy. Early bronchoscopy and bronchoalveolar lavage are important in ruling out infections. When the BAL fluid is bloody, alveolar hemorrhage should be strongly considered. Definitive diagnosis of sirolimus‐associated pulmonary toxicity requires a lung biopsy.
Conclusions:
A high index of suspicion is required of all clinicians involved in the care of patients on sirolimus who present with new‐onset anemia and respiratory compromise. Because the offending drug can be fatal if not promptly recognized, its withdrawal is key to survival.
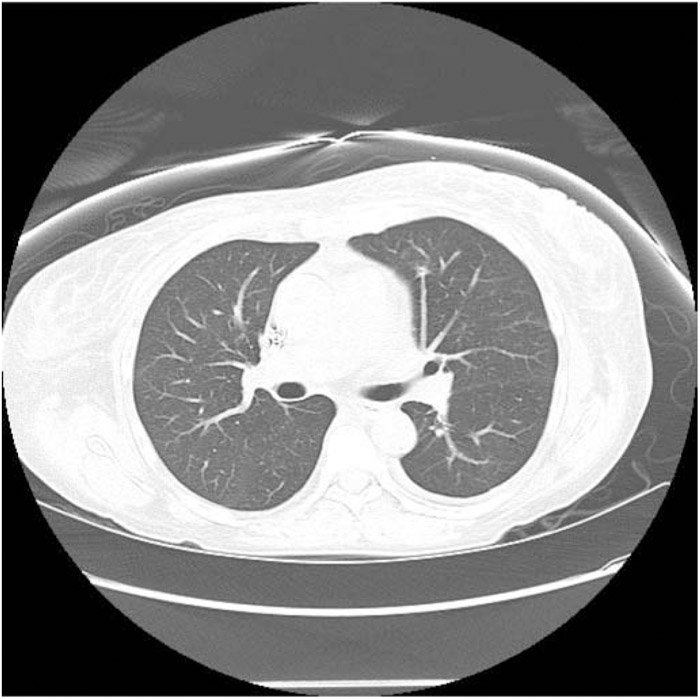
Computed tomography of the chest with complete resolution of opacities 11 days after discontinuation of sirolimus.
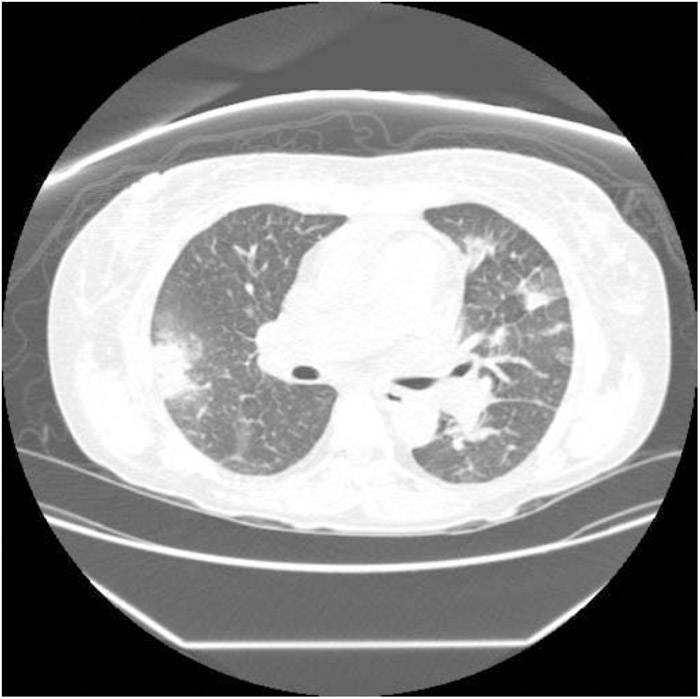
Computed tomography of the chest demonstrating bilaterall multi‐focal, irregular, nodular opacities.
Disclosures:
G. Popp ‐ none