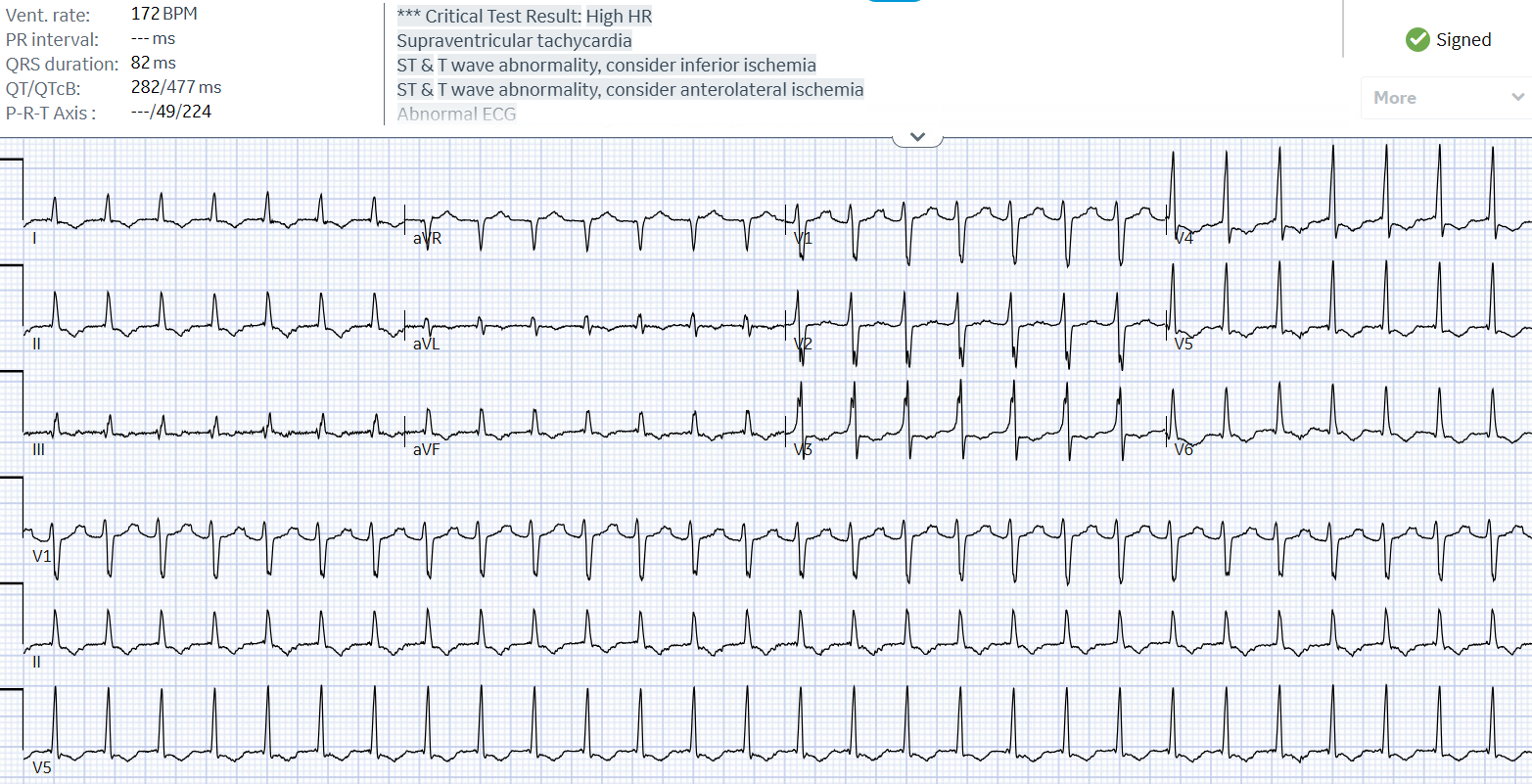
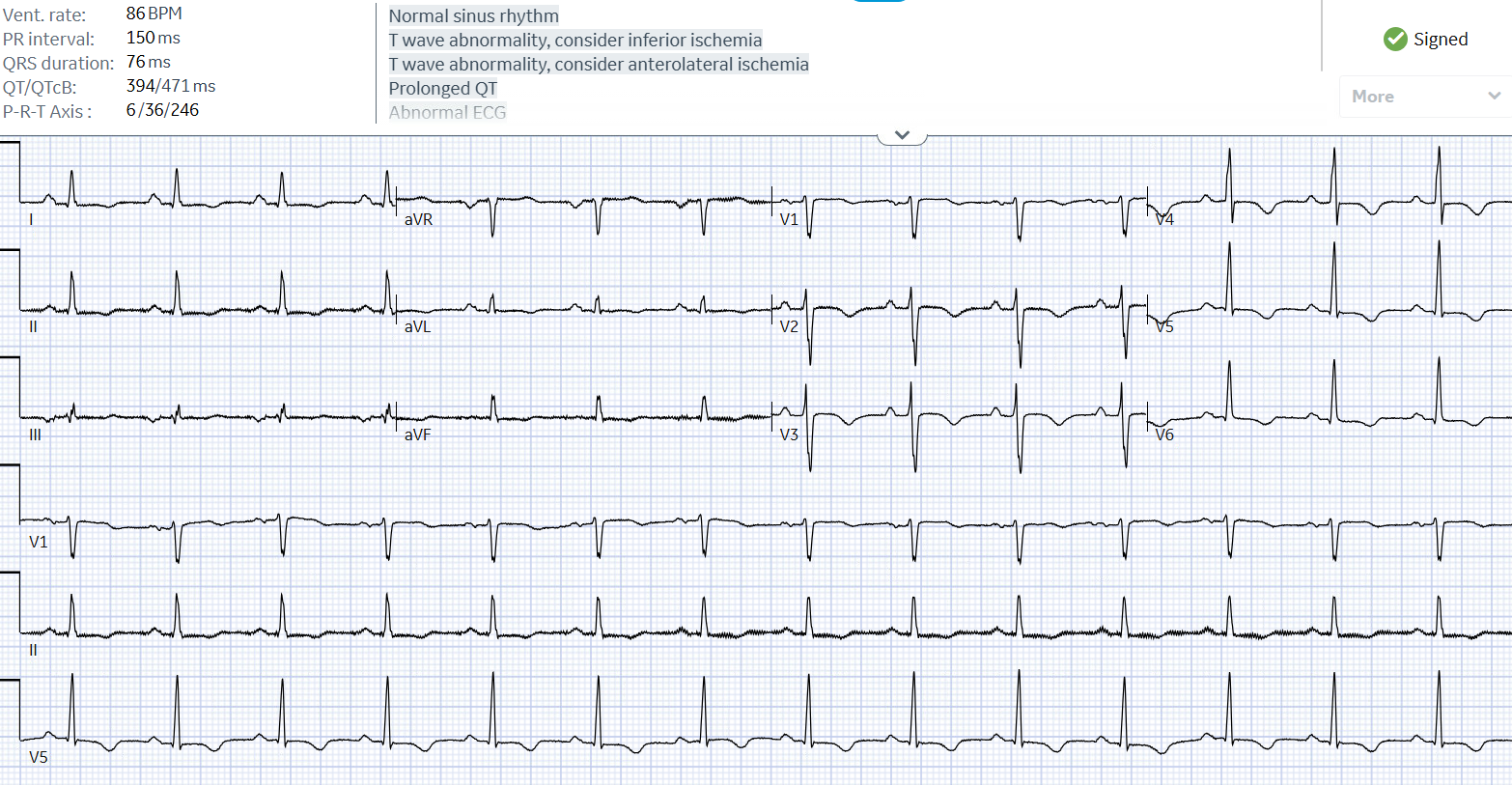
Case Presentation: 57-year-old male with a past medical history of nicotine dependence and concussion two weeks ago presented with supraventricular tachycardia (SVT) at another facility. He received Adenosine 6, 12, 12 mg and 2 L normal saline bolus, but did not convert and transferred to our facility for further management. Patient states that for the last 3 days he has been having abdominal pain, associated with nausea and one episode of vomiting. Denies any fever or sick contacts. Admission vitals showed tachycardia of 201 beats/minute and a blood pressure of 124/98. Examination was not significant. ECG showed a narrow complex QRS rhythm with retrograde P waves embedded inside the QRS complex consistent with a SVT pattern. Chest x-ray showed cephalization and bilateral pleural effusions. Labs revealed BNP 756 pg/mL, AST 143 U/L, and ALT 533 U/L. Patient presented with difficult to break SVT and was given Adenosine 6 mg and PO Lopressor 25 mg and IV Lopresor 5 mg, Adenosine 12 mg three times, and IV Cardizem 20 mg then 25 mg and 1 liter normal saline bolus, Adenosine 18 mg and finally converted back to sinus rhythm. Patient was admitted to the floors where he was noted to be in SVT again. Hemodynamically stable only complaining of chest pain. Patient denied all triggers of SVT such as alcohol, stress, etc. Of note patient was on room air, then nasal cannula and then placed on non-breather and did get hypoxic to 88% at some point. He received Adenosine 6, 12, and 18 mg. Also received IV Cardizem 10 mg push twice then started on drip. He received Amiodarone bolus and drip but was still in SVT. Patient was then transferred to the intensive care unit (ICU) for closer monitoring. He failed synchronized cardioversion at 150 and 250 Joules. He developed progressive hypoxic respiratory failure requiring anesthesia induction and intubation which was complicated by hypotension requiring pressor support. Bedside echocardiogram with severely reduced EF of 31-35%, global hypokinesis, and a thickened mitral valve, patient was found to have tachycardia induced cardiomyopathy. Patient spontaneously cardioverted just prior to central line insertion after intubation. Patient was eventually extubated and transferred to another facility and was successfully ablated for left sided wolff-parkinson-white (WPW) pathway. He was discharged on Losartan, Dapagliflozin, Spironolactone, and Bisoprolol. He will follow up in 4-6 months to reassess his ejection fraction after being on guideline-directed medical therapy.
Discussion: SVT is generally easy to treat, with 30% terminating with vagal maneuvers and upwards of 60% terminating with adenosine or other antiarrhythmics. Cardioversion is rarely required to terminate SVT. However, Cardioversion is the preferred treatment for unstable patients with WPW syndrome. Delta wave was not present on initial ECG for our patient, but further studies later completed by Cardiology-EP revealed he had left sided WPW pathway. Ablation of the accessory bypass tract, rather than antiarrhythmic medications, is first-line therapy for patients with WPW syndrome. Patients with Atrial fibrillation and WPW should not receive calcium channel blockers, β-blockers, or digoxin; such treatment may convert Atrial fibrillation to Ventricular tachycardia or Ventricular Fibrillation.
Conclusions: It is important for hospitalists to note the preferred treatment for unstable patients with WPW syndrome is cardioversion not antiarrhythmics! Ablation of the accessory bypass tract is first-line therapy for patients with WPW syndrome.