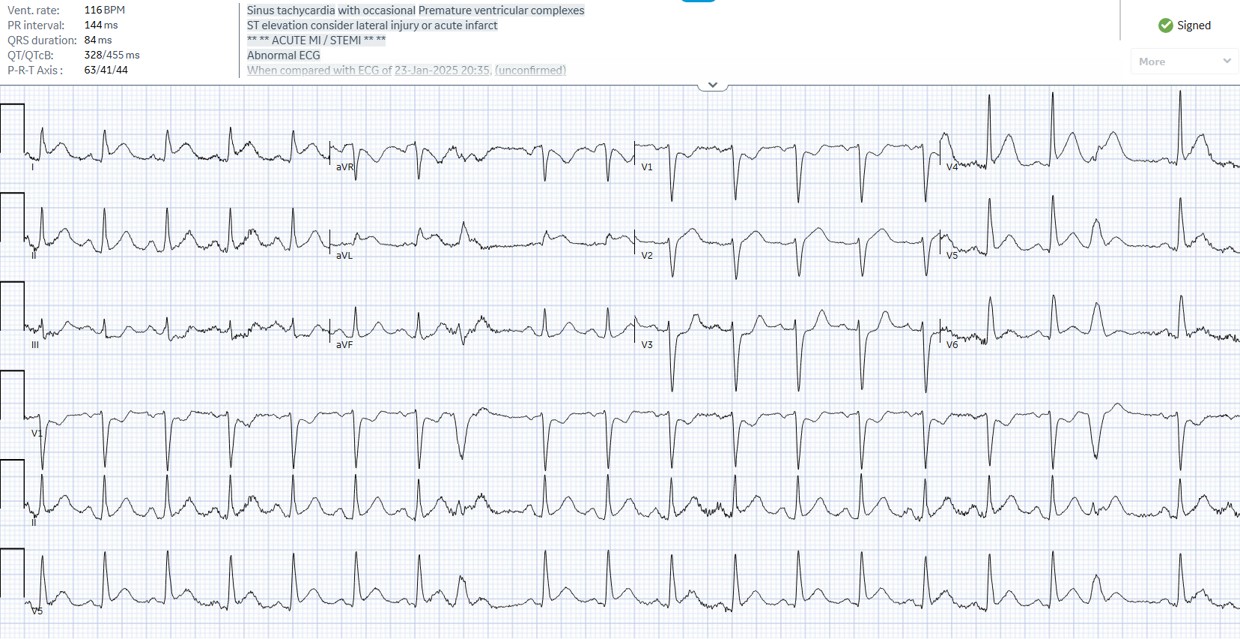
Case Presentation: A 77-year-old man with hypertension presented with 7 weeks of diarrhea and was found on colonoscopy to have a large, circumferential, friable rectal mass. Biopsy revealed poorly differentiated mucinous adenocarcinoma with signet-ring cell features arising from a tubulovillous adenoma, staged as T4N2M0. Neoadjuvant therapy was initiated with modified FOLFIRINOX, including a 48-hour continuous infusion of 5-fluorouracil (5-FU). Approximately 28 to 30 hours after starting the infusion, he developed acute chest discomfort, dyspnea, hypoxia (SpO₂ 74%), bilateral rales, transient ST-segment elevations, troponin of 315 pg/mL, and radiographic evidence of moderate pulmonary edema with small pleural effusions. Echocardiography showed severe global hypokinesis with LVEF 25%, while urgent coronary angiography demonstrated patent coronaries with only mild non-obstructive disease.
Discussion: The clinical picture (angina at rest, reversible ST elevation, troponin leak, Takotsubo-like severe biventricular dysfunction, flash pulmonary edema, and completely normal coronaries) was diagnostic of 5-FU-induced coronary vasospasm with secondary cardiomyopathy. Cardiotoxicity from 5-FU is well described (incidence 1 to 8%) and is significantly more common with continuous infusion than bolus administration, as the prolonged exposure promotes endothelial dysfunction and direct smooth-muscle spasm. After cessation of the infusion, aggressive diuresis, and supportive care, cardiac function normalized spontaneously without initiation of guideline-directed medical therapy for heart failure. Re-challenge was successfully performed using bolus 5-FU (over 1 hour) with prophylactic vasodilator therapy (amlodipine and isosorbide mononitrate), and no further cardiotoxicity occurred.
Conclusions: This case illustrates the potentially life-threatening but often reversible nature of 5-FU cardiotoxicity, even on first exposure and in patients without known coronary disease. Continuous-infusion schedules carry the highest risk. Prompt recognition, immediate discontinuation of the drug, and supportive care lead to rapid recovery in most cases. Importantly, the majority of patients can safely continue fluoropyrimidine-based therapy with a modified approach (bolus dosing plus prophylactic calcium-channel blockers and/or long-acting nitrates), allowing completion of potentially curative treatment for rectal cancer without permanent switch to less effective alternatives. Clinicians should maintain a high index of suspicion for cardiac symptoms during the 48-hour 5-FU infusion window.