
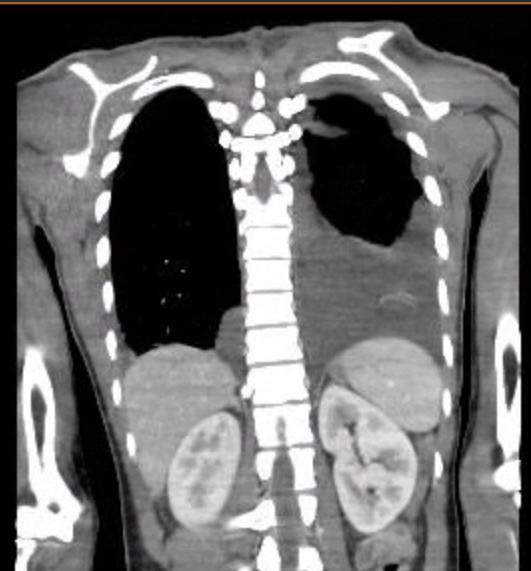
Case Presentation: A 30-year-old male with pre-diabetes and vitamin D deficiency presented to the emergency department with a two-week history of fever, watery diarrhea, sore throat, left shoulder pain, and bilateral ankle and knee arthralgias. On arrival, he was febrile (101.8°F), with laboratory findings revealing neutrophilic leukocytosis (WBC 33.6 x 10³/µL), markedly elevated inflammatory markers (ESR >130 mm/hr, CRP 29.5 mg/dL, ferritin 1019 ng/mL), lactic acidosis (lactate 2.5 mmol/L), procalcitonin 0.94 ng/mL, and elevated CPK (563 U/L). TSH remained normal (1.16 IU/mL). A respiratory pathogen panel (BioFire) detected enterovirus/rhinovirus, and chest CT revealed large bilateral pleural effusions with minimal abdominal free fluid. Empiric antibiotics were started. Infectious disease workup, including blood cultures, CMV serologies, Leptospira antibody, and QuantiFERON, was negative. Early anti-EBV IgG was positive with negative IgM. Autoimmune screening showed negative anti-cardiolipin, ANA, dsDNA, RF, and anti-RNP, but weakly positive anti-SSA (24 units), alongside positive anti-CCP and ASMA. Complement levels were elevated (C3 183 mg/dL, C4 26 mg/dL), though no Sjögren’s disease symptoms were present. Thoracentesis confirmed an exudative effusion without infection, leading to antibiotic discontinuation. Based on clinical, laboratory, and exclusionary data aligning with Yamaguchi criteria, adult-onset Still’s disease (AOSD) was diagnosed. Initial naproxen provided limited relief within 48 hours, but prednisone therapy led to complete symptom resolution.
Discussion: Adult-onset Still’s disease (AOSD), a rare systemic inflammatory disorder, is characterized by polyarthritis, fever, evanescent rash, and elevated inflammatory markers, with an incidence of 0.16–0.4 per 100,000 annually [1-2]. Pleural effusions occur in 30-40% of cases, adding diagnostic complexity [3]. The presence of weakly positive autoantibodies, such as anti-SSA/Ro-52 or ANA, though uncommon, has been sporadically reported, though its significance remains unclear [4-5]. This case, meeting Yamaguchi criteria without overlapping rheumatologic features, exemplifies the diagnostic challenges of atypical AOSD presentations, necessitating a thorough differential workup.
Conclusions: This case highlights the intricate diagnostic landscape of AOSD, emphasizing the need for further research to unravel its pathophysiological mechanisms and develop standardized treatment guidelines for atypical manifestations, ultimately improving patient care.
.png)