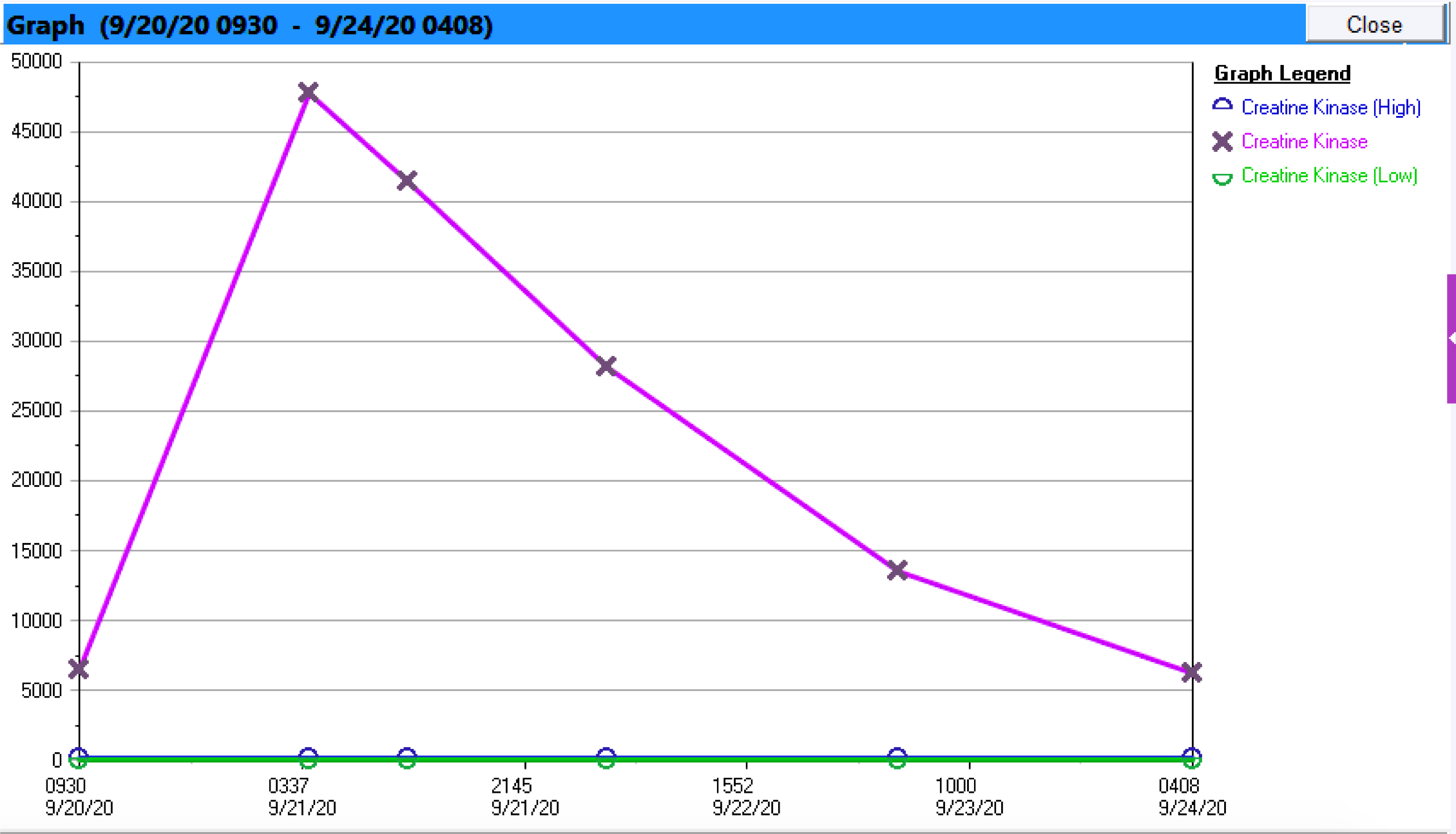
Case Presentation: A previously healthy 43-year-old AAM presented with weakness and dyspnea for 6 hours. Patient suddenly developed dull neck pain while resting at home. Hours later the pain progressed to weakness and aching in all extremities, trunk, and abdomen. He woke gasping for air secondary to chest tightness and noted having dark brown urine. He denied precipitating factors including trauma, increased physical activity, injury, medication use and herbal therapies. Patient works in construction spending many daylight hours outdoors. On exam, he was hypertensive with dry oral mucosa and decreased range of motion limited by pain. His creatinine kinase (CK) was 6444 with urinalysis revealing myoglobinuria. Renal function was at baseline with negative urine toxicology. However, he had notable AST of 1432, ALT 318, and normal alkaline phosphatase. His rhabdomyolysis was attributed to hypovolemia, and he was started on aggressive fluids. Further questioning on day 2 revealed that, prior to presentation, he drank a gallon of water daily. He denied dietary changes but admitted to eating a large serving of buffalo fish two hours prior to symptom onset. All others who consumed the fish were asymptomatic. Patient’s CK up-trended with a peak of 47,000 then improved with bicarbonate infusion and fluids. His CK continued down-trending with concomitant improvement in his pain and eventual discharge.
Discussion: Rhabdomyolysis is caused by the breakdown of skeletal muscle and release of intracellular contents. Clinically myalgia and dark urine are common presenting symptoms with elevation in CK and myoglobin. Broad etiologies include: traumatic, non-traumatic exertional, and non-traumatic non-exertional. In a patient working outdoors, it is appropriate to consider the horse when seeing the hoof-prints of rhabdomyolysis. Patient history becomes invaluable when distinguishing between non-traumatic exertional and non-traumatic non-exertional causes. However, especially in the southern U.S where freshwater fish consumption is common, it is important to consider zebra as well. Haff disease is precipitated by ingesting toxins in freshwater fish including eel, crayfish, buffalo fish, and carp. The toxin is likely heat-stable as in many cases, occur in the setting of cooked fish consumption.
Conclusions: In patients with rhabdomyolysis without an obvious inciting factor, clinicians should broaden their differential to include Haff disease. This becomes important as not all consumers develop rhabdomyolysis suggesting a multifactorial system in which affected patients may be predisposed to recurrent disease.