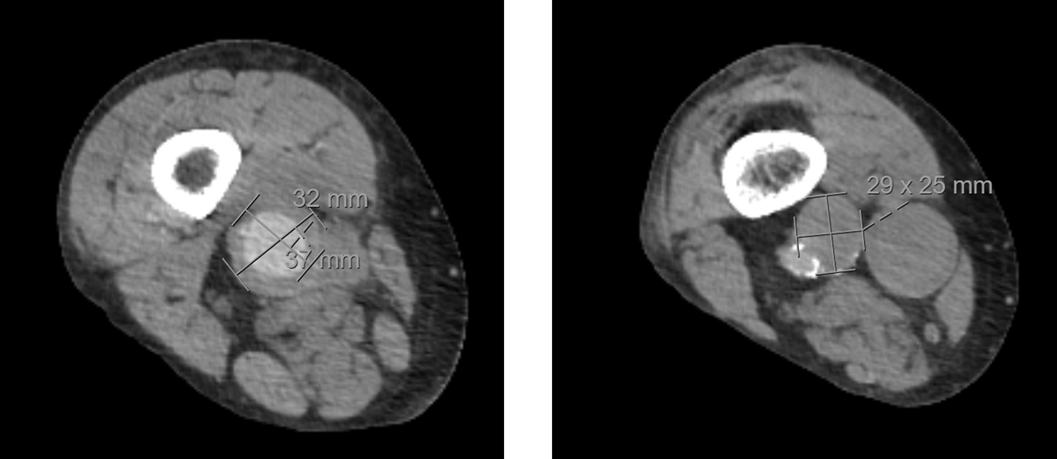
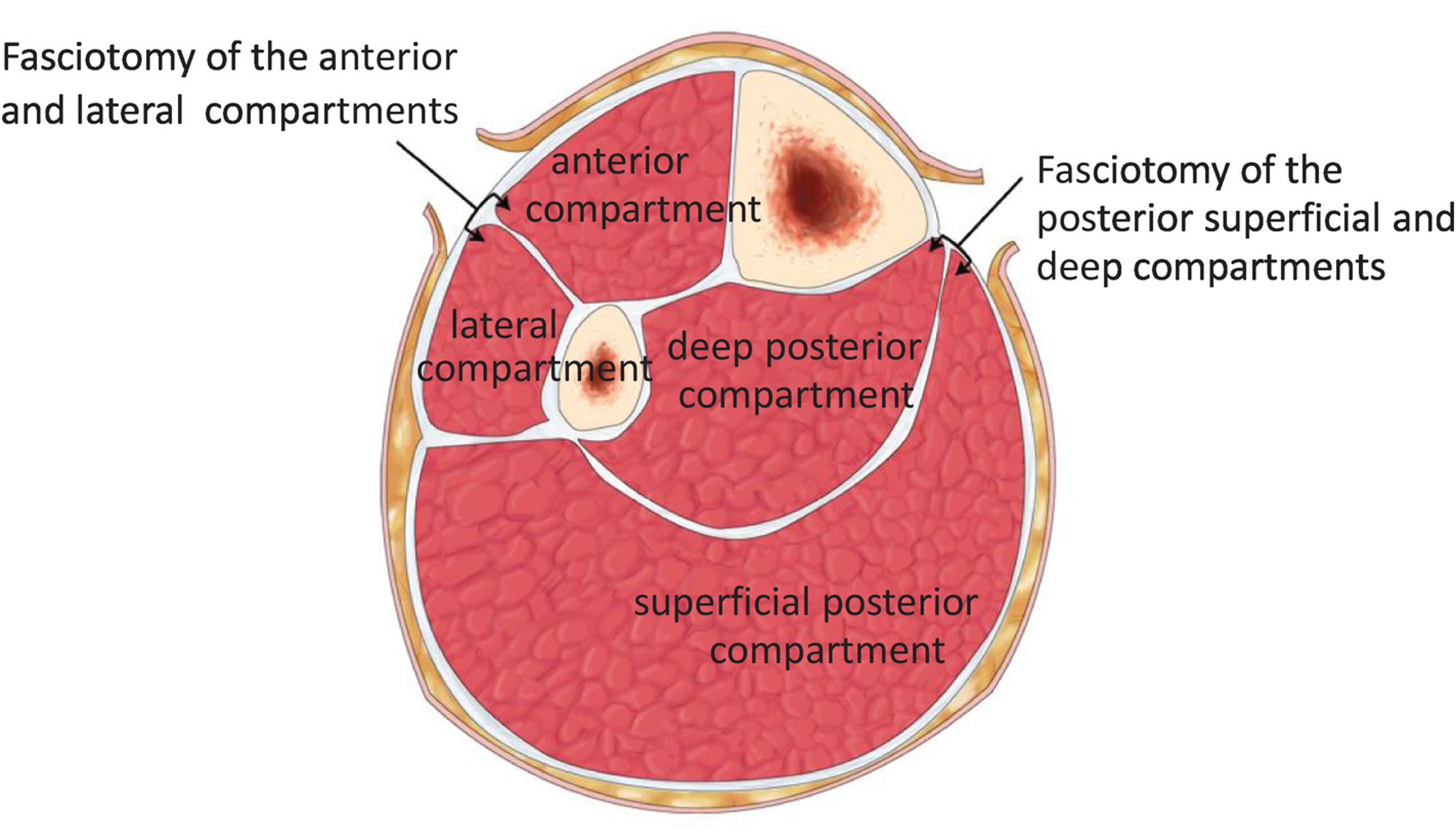
Case Presentation: A 63-year-old man presented with two-day history of right leg swelling, lacy rash, numbness in the right toes, and progressive pain. History includes hyperlipidemia, tobacco use disorder, recurring arterial aneurysms status post remote aortic aneurysm repair, peripheral vascular disease status post aortobifemoral bypass and left femoral to popliteal bypass. He had delayed capillary refill but bounding dorsalis pedis and posterior tibialis pulses. He had a violaceous reticular rash involving the skin from his knee down to his ankle. He had diminished ankle dorsiflexion and plantarflexion. He was exquisitely tender particularly over the anterior and superficial posterior compartments though with distensibility.Venous duplex was negative for DVT. Arterial duplex revealed triphasic flow into the foot. CTA Abdomen/Pelvis with bilateral runoff demonstrated distal superficial femoral and popliteal artery saccular aneurysm with thrombosed aneurysm at the superior margin of the right popliteal fossa. Creatine kinase was 15,284 IU/L. IV fluids and IV heparin were initiated. Vascular surgery was consulted and given initial distensibility on exam, compartment syndrome was initially not favored but recommended transfer to a quaternary care facility. On arrival, the anterior compartment was no longer distensible and he was taken for emergent four compartment right lower leg fasciotomy. The anterior and superficial posterior compartments were without overt myonecrosis but the muscle was minimally reactive. Subsequently, he underwent angiogram, endovascular repair of superior femoral and popliteal artery aneurysms. His course was complicated by hemorrhagic shock while on a heparin drip requiring IR embolization of a jejunal arterial branch with subsequent development of ileus. His ileus later resolved and underwent closure of the fasciotomy wounds. Over months of rehabilitation, the patient regained full dorsiflexion and plantarflexion and is no longer requiring a cane to ambulate.
Discussion: The diagnosis of impending compartment syndrome was delayed in this patient secondary to an unrecognized association of arterial aneurysm with rhabdomyolysis and compartment syndrome. Case reports of abdominal aortic aneurysm rupture and repair have established an association with compartment syndrome but this was attributed to post-operative fluid management. Rhabdomyolysis is a recognized precursor to compartment syndrome. Ischemia from arterial compression can result in rhabdomyolysis. The patient’s livedo reticularis of the skin could represent a manifestation of microvascular ischemia. We propose that the patient’s popliteal saccular aneurysm with thrombosed aneurysm may have resulted in direct ischemia. Further, being at the level of the popliteal fossa, extrinsic compression of the surrounding capillary bed may have exacerbated the microvascular ischemia. This was not ameliorated by medical management with a heparin drip as the cascade of ischemic muscle injury was already underway.
Conclusions: This case highlights that lower extremity arterial aneurysms can cause rhabdomyolysis and compartment syndrome.