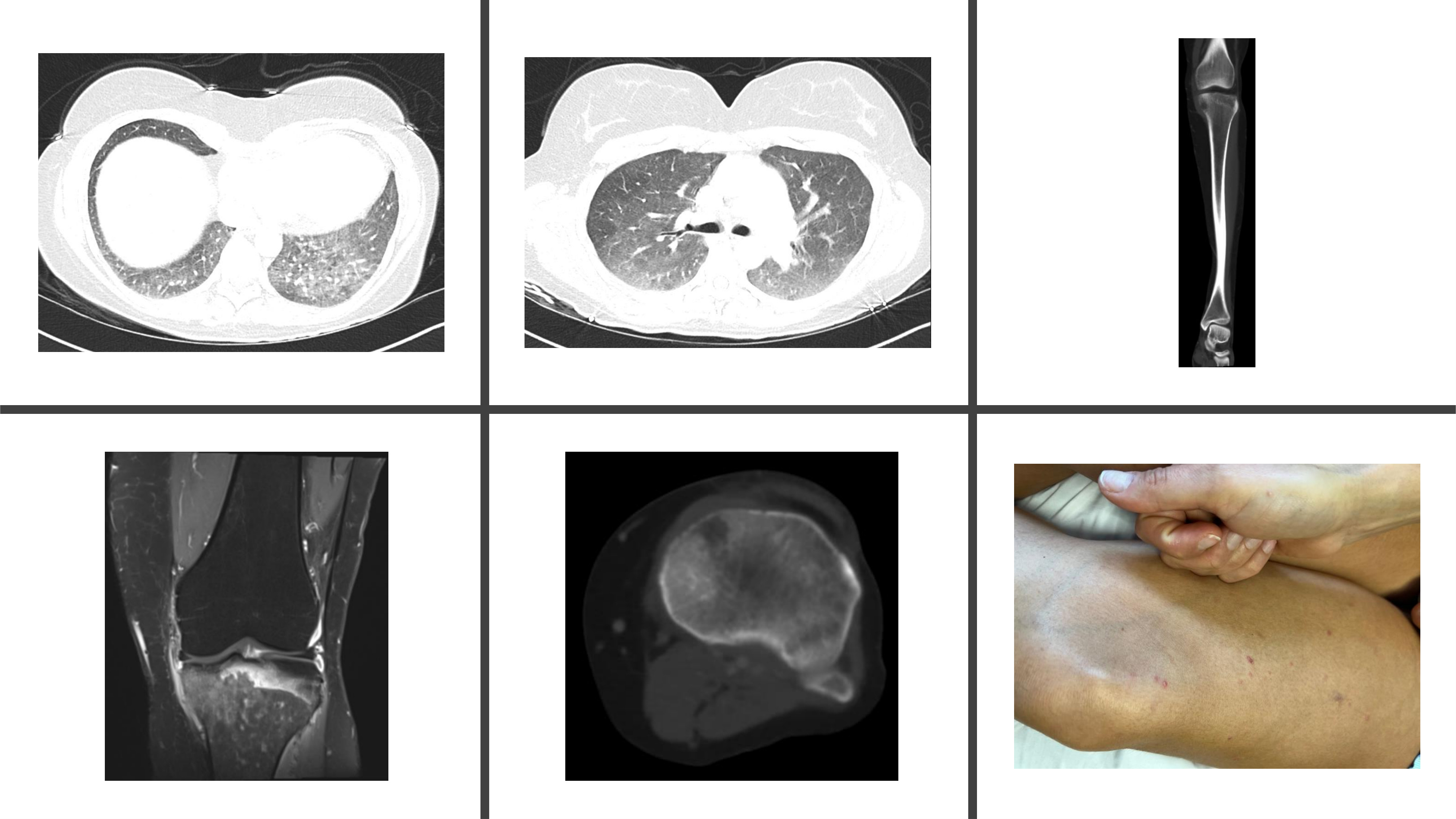
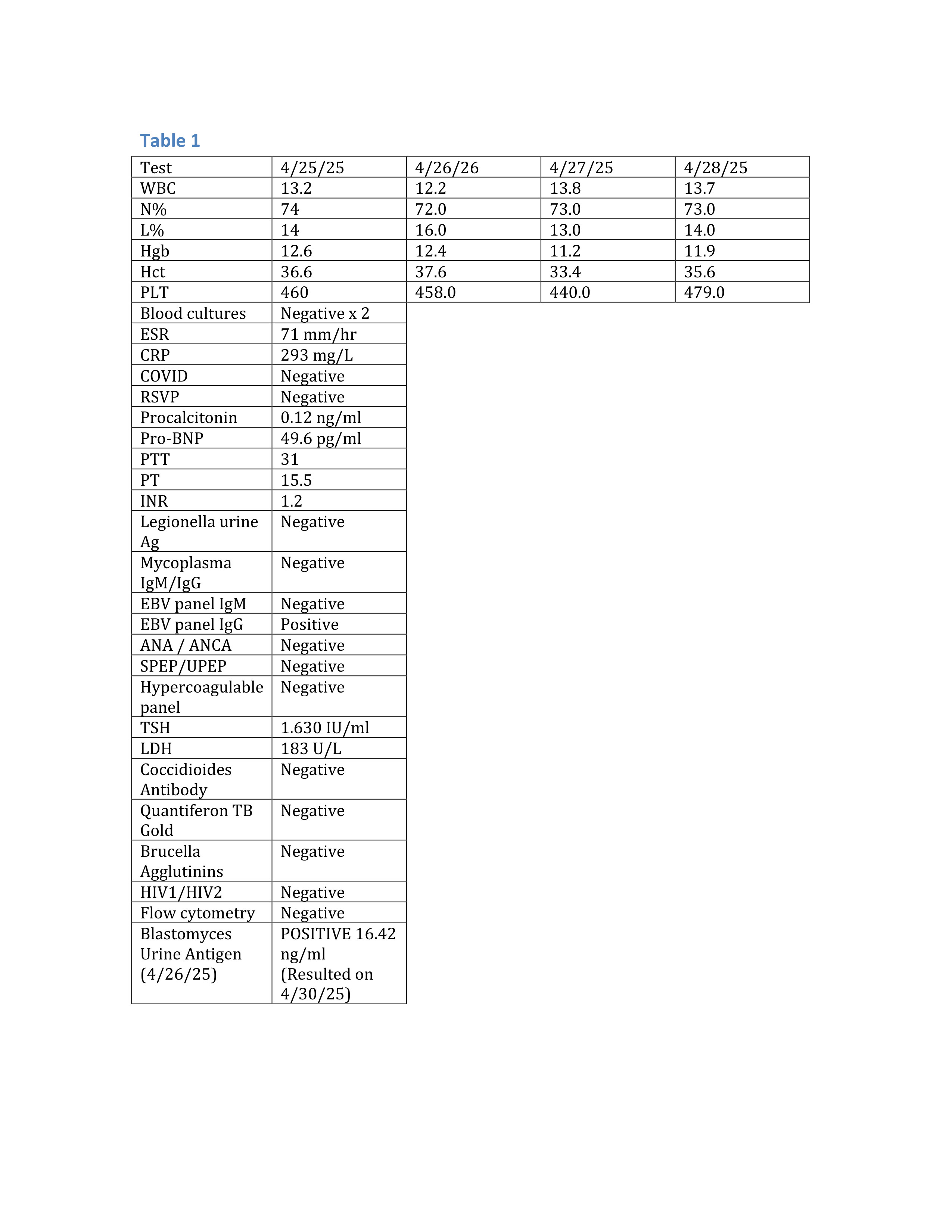
Case Presentation: A 46-year-old woman with a history of migraines presented with left knee pain after a gym session. MRI revealed diffuse marrow edema of the proximal tibia, medial collateral ligament thickening, popliteus muscle strain, and joint effusion. Concern for a stress fracture led to conservative management with rest and analgesics.Days later, she developed fatigue, malaise, and exertional dyspnea. On evaluation, she was hypoxic with fine crackles at the left lung base. Chest CT showed ground-glass opacities without pulmonary embolism (Figure 1A). Doppler ultrasound revealed acute thrombosis of the mid soleal vein. She was started on apixaban and empiric antibiotics for presumed pneumonia.Despite treatment, symptoms worsened. Labs showed leukocytosis, elevated CRP and ESR. Repeat tibial imaging revealed a 9 mm lytic lesion with cortical breakthrough and periostitis (Figure 1B). MRI raised concern for malignancy (e.g., lymphoma or multiple myeloma). Hematologic workup, including serum/urine immunofixation and skeletal survey, was negative for monoclonal gammopathy or additional lesions.Given systemic symptoms and exposure to renovation sites, infectious disease consultation was obtained. Extensive testing for EBV, Histoplasma, Brucella, Coccidioides, and TB was negative, but Blastomyces urine antigen was positive (Table 1). She later developed skin lesions (Figure 1C), and antifungal therapy with amphotericin B was initiated.
Discussion: Blastomycosis is a systemic fungal infection caused by Blastomyces dermatitidis, endemic to North America, especially the Great Lakes and Mississippi/Ohio River valleys. Extrapulmonary dissemination occurs in 25–40% of cases, commonly affecting skin, bones, and the genitourinary tract. Bone involvement is rare and often misdiagnosed. It typically presents with localized pain and swelling, sometimes mimicking malignancy or bacterial osteomyelitis. Lower extremities, ribs, and vertebrae are frequently affected. A Canadian series of 45 cases found 73% had a single bone lesion, 64% had pulmonary involvement, and 22% had trauma at the infection site. Radiographically, bone blastomycosis presents as destructive, lytic lesions that may mimic malignancy, tuberculosis, or bacterial osteomyelitis. Early imaging may be normal or show subtle osteopenia. As disease progresses, eccentric lucencies with well-defined or diffuse borders may appear, sometimes accompanied by soft tissue abscesses or joint involvement. Vertebral disease may present with contiguous paravertebral abscesses.Treatment depends on severity. Itraconazole is first-line for mild-to-moderate disease. Severe or disseminated cases require amphotericin B followed by oral azoles. Alternatives include voriconazole or posaconazole for itraconazole intolerance.
Conclusions: We present a case of a common musculoskeletal complaint that evolved into a rare diagnosis of disseminated blastomycosis with osteoarticular, pulmonary and cutaneous manifestations. The initial presentation mimicked a stress fracture and neoplastic process, highlighting the importance of considering fungal infections in the differential diagnosis, especially in endemic areas or in patients with relevant exposures. Early recognition and initiation of appropriate antifungal therapy are essential for optimal outcomes.