
Background: Large academic medical centers (AMCs) increasingly rely on interfacility transfers to affiliated community sites to optimize bed capacity and resource allocation. Despite this trend, the characteristics and safety outcomes of patients selected for such transfers remain poorly understood. At our institution, a hospitalist triage physician evaluates patients in the AMC emergency department (ED) for potential transfer to an affiliated community hospital. When the patient and family assent, the patient is transferred and admitted to the hospitalist team at the affiliate site for continued inpatient care. Given a rapid increase in transfers over a short period, an evaluation of patient safety of this process was warranted.
Methods: We conducted a retrospective chart review to characterize patients transferred between the AMC and community hospital and to assess associated clinical outcomes. During the study period, the community hospital used Cerner and the AMC used Epic. A total of 651 patient encounters were analyzed using data extracted from both electronic health record systems. Variables included demographics (patient-reported sex, race, age, and primary language), clinical characteristics, readmission rates, and quality and safety metrics (code blue activations, rapid response calls, hospital-acquired complications—including delirium, infections, and falls—and restraint use). The Institutional Review Board (IRB) reviewed the project and determined that it did not constitute human subjects research.
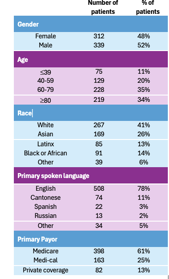
Results: A preliminary analysis of 40 randomly selected patient encounters from August 2024 to August 2025 identified no avoidable returns to the tertiary care center, no episodes of clinical deterioration during transfer, and no unplanned ICU admissions or other adverse events. Within this subset, there was one death and a 30-day readmission rate of 7.5%.We subsequently conducted a comprehensive analysis of all transferred patients during the study period. Demographic characteristics (Table 1) and safety-related metrics (Table 2) were extracted directly from the electronic health record. The average time from the tertiary care center ED to arrival at the affiliate hospital was 13 hours, and the mean length of stay at the affiliate hospital was 4.5 days. Over the one-year study period, 27 patients returned to the AMC ED after discharge and were readmitted, subsequently being transferred again to the community hospital. The 7-day and 30-day readmission rates were 4.1% and 8.7%, respectively. There were two deaths, corresponding to a mortality rate of 0.31%
Conclusions: Results show that patients transferred from an AMC to an affiliated community hospital experienced low rates of safety events. We plan to conduct manual chart reviews of all patient encounters to analyze narrative data and further evaluate specific clinical outcomes, including causes of morbidity and mortality, delirium, and consultant utilization.
.png)